On August 16, 2016, the HHS Departmental Appeals Board (DAB) issued a decision related to CMS’ authority to revoke a Medicare supplier’s billing privileges. The DAB is the fourth and final level of administrative appeal within the Department of Health and Human Services.
Factual Background
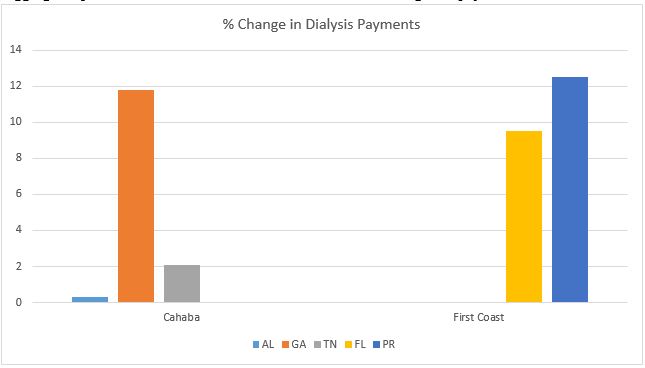
The case involved John P. McDonough III, Ph.D., a clinical psychologist residing in Florida, and two of his affiliated medical practices, Geriatric Psychological Specialists and Geriatric Psychological Specialists II. In October 2014, First Coast Service Options, Inc., the Medicare Administrative Contractor for Florida, notified McDonough and both medical practices that their Medicare billing numbers were being revoked for alleged abuses of their billing privileges. Specifically, First Coast indicated that data analysis had revealed that the three suppliers had submitted a total of 420 claims for deceased beneficiaries over an approximately two-year period.
McDonough and his two medical practices appealed for a reconsideration of the revocation of their billing privileges, which was denied in February 2015. The suppliers then appealed for an ALJ hearing. The suppliers conceded that they submitted more than 200 claims for beneficiaries that were deceased on the date of service. However, they attributed these claims to data-entry errors and other clerical mistakes. The suppliers argued that these were simple billing errors, representing a small percentage of the tens of thousands of claims they submitted during this period of time. In December 2015, the ALJ issued his decision. While the ALJ seemingly accepted the suppliers’ explanation that these were billing errors, and that there was no intent on the part of the suppliers’ to submit false claims, the ALJ nevertheless upheld the revocation of their billing privileges. Citing previous DAB decisions, the ALJ held that the admitted submission of repeated claims for services to deceased beneficiaries due to “incorrect billing entries due to similar beneficiary names or Medicare numbers, and inadvertent typing errors” was not inconsistent with a finding that the suppliers’ had abused their billing privileges.
The suppliers’ then appealed to the DAB. In its decision, the DAB first noted that it has consistently rejected contentions that revocation required a finding that the supplier acted intentionally:
“The Board has long held that the regulation’s plain language does not require CMS to establish fraudulent or dishonest intent to revoke a supplier’s billing privileges under this section and that the regulatory language also does not provide any exception for inadvertent or accidental billing errors.”
The DAB then countered the suppliers’ argument that CMS never intended to revoke a supplier’s billing privileges for simple mistakes. They cited language from the June 27, 2008 final rule, where CMS stated revocation “is not intended to be used for isolated occurrences or accidental billing errors.” The DAB noted that CMS, in that same final rule, indicated that it would not consider the submission of three or more improper claims to be accidental. The DAB also noted that the relatively small percentage of erroneous claims was irrelevant, as the regulation does not require CMS to establish any particular error rate or percentage of improper claims.
The DAB held that since the record established that the suppliers’ had submitted more than 3 claims for deceased beneficiaries, CMS had met the requisite legal standard for revocation. Accordingly, the DAB upheld the revocation of the suppliers’ billing privileges.
Potential Impact on Ambulance Providers
The DAB’s decision effectively establishes a strict liability standard for revocations based on the submission of claims for deceased beneficiaries. The submission of three or more such claims over any designated period of time could constitute legal grounds for CMS to revoke a supplier’s Medicare billing privileges.
The implications of this decision should give every Medicare provider pause. However, given the nature of our operations, our industry needs to pay particular attention. The psychologist and therapists that were the subject of the above-referenced case saw patients on a scheduled basis, and spent many hours with each of their patients. This gave them ample time to obtain insurance information from each of their patients, and to confirm the accuracy of that information. Yet the suppliers’ still had more than 200 claims billed incorrectly.
EMS providers do not have that luxury. We frequently encounter patients on the street or at their home. Many of these patients do not have their insurance information on them at the time of transport. Even when the patient had this information on their person, under the stress of an emergency medical situation, the paramedic or EMT may not record this information accurately.
As a result, our billing offices spend a good portion of their time trying to verify a patient’s insurance. Unfortunately, some of the administrative “shortcuts” we have developed to address these problems create the potential to inadvertently submit claims for deceased patients. While there is nothing at present that suggests that CMS intends to expand the use of its revocation authority, we probably want to rethink these shortcuts.
An example you say?
Consider a transport of an elderly woman to the hospital in an emergency. The crew does not obtain the patient’s insurance information at the time of transport. However, they do obtain the hospital face sheet, which lists the patient’s social security number. To convert this social security number to a Medicare HIC#, we need to include a Medicare suffix. How would you go about doing that?
One option would be to ping the patient’s name, date of birth and SSN against an eligibility database. While effective, provider’s typically pay for these lookups.
Another option would be to simply guess what the applicable suffix might be, affix that to the SSN, and submit the claim. If it goes through, the provider guessed correctly. If it rejects as an invalid name and HIC# combination, the provider would know to try another suffix. So let’s assume the provider elects to use this option. Playing the percentages, the provider would likely add the “B” suffix, on the theory that, given her age, the woman likely qualified for Social Security Benefits (and therefore Medicare benefits) based on the work history of her spouse. But what if the provider was wrong, and the woman was the primary wage earner in her family? If that were the case, her suffix would likely be the “A.” Now imagine that her husband shared the same Social Security numerics, and that his suffix was the “B.” Further imagine that he has since passed, and the provider has now inadvertently submitted a claim for the dead husband.
Now imagine this happens three times in a year…
Another way we can inadvertently submit claims for dead patients is not using front-end verification. Many providers submit claims based off the insurance information they received at the time of transport (or from the hospital, nursing home, etc.), without any attempt to confirm its accuracy. These providers recognize that the insurance information will be correct more often than not. They are making the calculated decision that it is easier to deal with any issues after they have been identified by the payer. However, one reason an insurance can come back as invalid is because the crewmember recorded the HIC# incorrectly. For example, they may transpose a few digits (i.e., they wrote “1243” rather than “1234”). If the transposed HIC# relates to a deceased beneficiary, that would be captured by the data analytics used by the Medicare contractors.
The DAB’s decision is certainly troubling. However, I do not believe that our industry needs to overreact. Rather, I would encourage everyone to view the DAB’s decision as a starting point, and to re-examine their own billing and verification processes to see if there is anything they can do to reduce the likelihood of their organization every confronting this issue.
Have an issue you would like to see discussed in a future Talking Medicare blog? Please write to me at bwerfel@aol.com.