The 9 Line Company (www.the9linecompany.com) has launched a campaign to support EMS professionals who have lost their homes and are facing significant hardships due to the recent fires.
As you may know, The 9 Line Company is a training and education organization, working with EMS personnel and first responders nationally and globally. Here at LifeLine EMS, two of our own EMTs have lost everything in the Eaton Fire, and we are aware of others at different companies facing similar devastating circumstances.
When we couldn’t find an organized effort to address this specific need, we decided to create one through 9 Line. Through this campaign, any EMS personnel in Southern California who have lost their homes or are experiencing severe challenges can reach out to The 9 Line Company for assistance. Every dollar donated will go directly to helping these EMS heroes rebuild and recover.
Two of our EMTs are in this position and it breaks my heart.
Please feel free to share this initiative. Many have asked how they can help, and contributing to this campaign would make a meaningful impact.
New Funding Available for Rural Health Care Services Outreach Program
Apply by January 27, 2025
The Rural Health Care Services Outreach Program (Outreach) is open and accepting applications for the program’s 4-year period of performance (May 1, 2025-April 30, 2029). HRSA will make up to 50 awards to support rural communities to expand the delivery of health care services. These awards include:
An estimated 40 awards, each up to $250,000 per year, under the program’s regular track to support healthcare needs identified by the rural community applicant;
Up to 10 awards, each up to $300,000 per year, under the program’s special track to address the underlying factors that drive rural health disparities related to heart disease, cancer, unintentional injury/substance use, chronic lower respiratory disease, stroke, and maternal health.
Eligible applicants include all domestic public and private, nonprofit, and for-profit entities with demonstrated experience serving, or the capacity to serve, rural underserved populations. Applicants are also required to propose projects that serve exclusively HRSA-designated rural areas and be a part of a network comprised of three or more organizations with at least two-thirds or 66% percent network organizations physically located in a HRSA-designated rural area.
Successful Outreach Program awardees will: 1) expand the delivery of health care services to include new and enhanced services exclusively in rural communities; 2) use innovative, evidence-based and promising practice models to inform their approach to addressing needs specific to their community; 3) demonstrate health outcomes; and 4) plan for sustainability after grant funding ends.
Examples of previously funded projects under this program are available at this link. Applicants may also benefit from the availability of Evidence-Based Toolkits for Rural Community Health which are informed by previous program investments by the Federal Office of Rural Health Policy and the Rural Health Information Hub.
For more information about this funding opportunity, contact the Program Coordinator, Mew Pongsiri, at RuralOutreachProgram@hrsa.gov.
It is with great sadness the American Ambulance Association announces the passing of long-time member and leader Joe Huffman.
Obituary
Joe (Joel Claude) Huffman, a long- time member of the American Ambulance Association Board of Directors answered his Last Call July 1, 2019. after a long battle with Leukemia.
Born August 11, 1954, Mr. Huffman died at his home in Garland surrounded by his family and friends.
From his funeral service at First United Methodist Church of Richardson Mr. Huffman was taken in an ambulance rather than a hearse to Grove Hill Memorial Park in Dallas The funeral procession included 17 ambulances and 14 command vehicles, as well as a police honor guard and other mourners. Following a rendition of Amazing Grace on bagpipes first responders performed The Last Call ceremony.
A licensed paramedic, Mr. Huffman was also active in professional organizations, serving on the board of directors of American Ambulance Association for 18 years and as a member many more years.
He served as president of the Texas Ambulance Association for two years, and was on its executive board many of the more than 30 years he was a member
While president of the Texas Ambulance Association, Mr. Huffman was instrumental in drafting legislation which established standards for Emergency Medical Services in Texas.
At the time of his death Mr. Huffman had been Special Events Coordinator of American Medical Response for 16 years, providing standby service at Cowboy Stadium, ATT stadium, the Cotton Bowl, Lone Star Park in Grand Prairie as well as many others.
Mr. Huffman had worked at the State Fair of Texas First Aid Station for 45 years, never missing a day. Twenty-three of those years he was director of the station. He formerly owned Dallas Ambulance for 11 and a half years. Adding these years of service, Mr. Huffman packed 142 ½ years of service into the 64 years and 10 months of his life.
The son of a locomotive engineer, Mr. Huffman was an avid collector of model trains and railroad memorabilia. He was a lifetime member of the American Museum of Railroads at Frisco, Tx., where he has donated his extensive collection of model trains and railroad memorabilia.
Mr. Huffman graduated from W.W. Samuel High School, attended SMU and earned an A.A. degree at Eastfield Community College.
Memoriam gifts may be sent to the Leukemia and Lymphoma Society of North Texas.
A lifelong resident of Dallas, Mr. Huffman is survived by his Beloved Cheryl Hale of Tyler; a sister, Joyce Huffman Prock, of Bedford; two brothers, Jack W. Huffman and his wife, Donna of Richardson; and James (Jimmy) Huffman of Dallas.
Also, four nieces, Dana Huffman and Melanie Bullock of Richardson; Leslie Prock Norton and husband Andrew, of Bedford; and Angel Marie Huffman Dellinger and husband, Scott, of Crandall. Two nephews Erik Prock of Ft. Worth and Jason Huffman, of Richardson, who is deceased. Great nieces Jaylyn Scott Norton of Bedford; Denise Marie Dellinger of Crandall; and Caroline Huffman of Richardson. Three great nephews, Jack Michael Huffman of Richardson; Dylan Scott Dellinger and Devon Scott Dellinger of Crandall. He was preceded in death by his parents, James J. (Happ) Huffman and Florence Bolin Huffman.
The transcript below was lightly edited for clarity.
Amanda Riordan: Thank you for joining us today. My name is Amanda Riordan, and I am the vice president of member services for the American Ambulance Association. I’m also the administrator for the Professional Ambulance Association of Wisconsin. I’m so happy to have the opportunity to interview John Eich, the director of the Wisconsin Office of Rural Health. John is an exceptional contributor to rural health in Wisconsin. He’s also a sterling advocate for the power of EMS to assist with public health in the least accessible areas of Wisconsin. I’ll ask John a couple of questions today about the recent Rural EMS Listening Sessions that he conducted in a number of areas across the state. John, thanks again for joining us. Would you mind telling me a little bit about your background and how you became the director of the Wisconsin Office of Rural Health?
John Eich: I appreciate your inviting me to talk about some of our programs, so thank you. I took a bit of a wandering path: I’ve done everything from carpentry and marketing to social work with homeless teens. I found my way to community [service] down in southern New Mexico. I caught the bug there working on behalf of the community and society at large. When I moved back home up to Wisconsin—I grew up in a rural area here in southern Wisconsin—I saw an opening and at the Office of Rural Health. I’ve been on board ever since, and it’s a lot of fun.
Amanda Riordan: Thanks so much. And we’re so glad you took the position. Would you mind sharing a little bit about why EMS is so important to rural health?
John Eich: If you’re not familiar with an office of rural health, we receive mostly federal funding to work on the state level. There’s an office in every state in the nation. Here in Wisconsin, we are funded mostly, I would say, to work with rural hospitals and EMS, and we find that EMS is one of the areas of greatest need. Every piece of the healthcare delivery system has its challenges and its strengths. EMS, I think by the nature of having formed itself—at least rural EMS formed itself—around the model of volunteer services. In my estimation, it has sort of painted itself into a corner. It started when medicine was not as complicated, and when populations, were not expecting as much. You were helping out your neighbors by getting somebody to a hospital. It has since evolved in a good way.
[EMS has] evolved into a healthcare profession. And so there are a lot more demands. There’s a lot more education; continuing education, learning new techniques that are lifesaving. Society depends on it. But that means that these volunteer services that started off small are under increasing pressure. That’s why we are trying to dedicate as many of our resources as we can to helping out that system within Wisconsin, and it’s paying great dividends. We’ve always really enjoyed our interactions with EMS. I think it takes a particular kind of person to do it. We just really enjoy our time with those who do the work. That led us to doing what we’re calling a “Rural EMS Listening Session.” So we did five of these sessions around the state in rural areas, and we intend to do a few more.
Part of the idea was that so often policy in general happens in urban centers. In EMS policy, because the state capital is down in the very southern part of the state and Milwaukee, the largest city is also down in the southern part of the state, the rural areas of the state (which most of the rest of it) tend to feel ignored or unheard. It’s much harder for them to participate. So if somebody has to drive five hours to go to a meeting that would take [a city resident] 15 minutes to drive to, that’s a disparity in access and it’s a disparity in having your voice heard. So we decided that it was important to go listening where rural EMS is practicing. So we did that, and are continuing to do so.
It’s been very eye opening. Obviously there was a lot that we expected to hear that we did hear. I mean, there’s, there’s not a lot new here. People in EMS know what the issue is as someone said these are the same ideas we’ve been talking about for the last 20 years or more. And that’s very true. We like to believe that it’s time for things to change. We’ve been talking about this long enough. Maybe we should do our best to push the issues forward. And that’s phase two of these listening sessions: take what we heard and get it into the hands of advocates, like the EMS associations, fire associations, et cetera, and other advocates like the Office of Rural Health that try to speak on behalf of the needs of EMS. I do think I’m optimistic that legislators want to help. When they’ve been presented with bills, they’re interested. Money is always an issue, but I would say that they definitely want to be part of a solution. So, it’s all of our jobs to make sure that they have the right solutions and presented to them.
Amanda Riordan: I think that’s a great segue to one of your other very popular innovative programs in Wisconsin. The Office of Rural Health actually helped put together the EMS at the Capital Day event in 2017. Would you mind telling us a little bit more about what that entailed and the groups that participated?
John Eich: Absolutely. So again, as we work with all parts of the healthcare delivery system, we work with hospitals and clinics and providers; physicians, PAs/physician assistants, nurse practitioners, the nurses that staff the hospitals and clinics and home health services. When we look at EMS, it always strikes me how it has a level of splintering that I don’t see in other professions. In other professions, they’ve managed to sort of circle the wagons and get on the same page and present a united face to push forward their vision and their legislative goals. EMS, for whatever reason. I’m not sure why it seems to have done the work but also, identified a number of differences. You can be a paid or career staffer versus a volunteer. You can work in a rural service versus an urban. You can be in fire versus EMS. You could be a Paramedic or you could be a Basic EMT or an Emergency Medical Responder. Each of those areas, each of those groups, sort of huddle and identify amongst themselves. I would like to see them working more cohesively together and I’m sure they would as well.
The effort that that led to an EMS Day at the Capital was to try and get all of the disparate groups together and on the same page. All of them had been working very diligently on the issues that were important to them, and I think there is a lot of overlap. As one of the participants said, “We can agree on a 80 percent of the issues, we may disagree about the 20 percent, but let’s work on the 80 percent and when we get that done, then we can disagree about the rest of them.”
So that was the goal that brought the groups together. So we were lucky to be able to get the two EMS associations in the state, the state fire chiefs, and the professional firefighters. The state EMS board joined in with us as well as they could, in more of a listening capacity. We created a wish list of legislative issues and a lot of it was centered around education: who we are and what we do. And we took that to the state capital. We had tremendous turnout and we had uniforms marching through the, through the offices of the legislature both in the Assembly and the Senate. I like to think we got their attention and we plan to, as I said, take what we’re learning from this rural EMS tour, connect with our urban allies as well, and get EMS advocacy on the same page so that they can do tremendous work together.
Amanda Riordan: It was truly exciting and a privilege to witness everything that happened in November 2017 when the Professional Ambulance Association of Wisconsin, Wisconsin State Fire Chiefs Association, the Professional Firefighters of Wisconsin, and the Wisconsin EMS Association, all came together with the help of your office, the Office of Rural Health, to speak with one voice when meeting with state legislators. I think that by working together they were able to present such an incredibly compelling message to legislators and to key staff that worked with legislators. I think a lot of times people are somewhat unaware that winning over the hearts and minds of critical legislative staff is almost as important as running to over the hearts and minds of legislators themselves.
With that in mind, and with all of the successes you’ve had helping execute your vision of moving EMS and rural health forward in Wisconsin, would you mind telling us a little bit about where you see the future of rural health going in your state, Wisconsin, as well as the country in general?
John Eich: I take it you mean in EMS terms. Because there’s a lot going on in healthcare, as you know! As far as EMS goes, I think the future of EMS care is not a wholly volunteer model. I think it is at least a hybrid model, and I think the industry needs to figure out how to make that transition. I think that’s going to be a difficult and painful transition. I think it’s going to take a lot of education to the local politicians who are used to having their services and frankly to be getting a pretty good deal.
We talked recently to a small community. It was a countywide meeting, but it was held in a small community that had been [served by] a volunteer service. They said they had a core group of about five people. The chief of the service had had volunteered 4,280 hours last year. The rest of his staff [had volunteered] around the 3000-hour level. They were proud of that, understandably. They were also somewhat reluctant to consider another model in their mind. They felt that they were just fine. When I look at that from the outside, I think, “What if one of you tears an ACL as you’re getting off the ambulance rig, what if two of you get the flu really bad? Which happens!” [What happens if] then there are two calls for EMS, at the same time, while two of your staff are bedridden. That’s three people to make all those calls. I struggle with the vision of that is as sustainable.
But when the local community looked at the numbers, they said, well, it looks like as far as the taxes go, that’s about $12 per capita. I was a little horrified, and asked “is that per year?” And they said, “Oh yeah, yeah, that’s per year.” I was struck by the fact that I pay more for Netflix per month than these folks pay per year to have two highly trained individuals show up with the latest technology to save the lives of their loved ones. I’m not criticizing that, but I do think there’s an opportunity there to really examine that in the daylight. And certainly when the board realized that and looked at it, there was a lot of sort of a flurry of questions back and forth. And is this true? On and on.
I think the nature [of the matter is that] if you can possibly put the question to a citizen in a grocery store as they’re walking out with their groceries, “How much would you pay per year in your taxes to have this kind of lifesaving service?” I don’t think the answer would be $12 a year. I think it would be more, but I don’t think most citizens or politicians have been given the opportunity to really look at. I think they assume it’s already paid for. It’s part of their taxes. I think they assume that Paramedics just show up at their door. They don’t necessarily know the difference between a Paramedic and a Basic EMT or EMR. They have a great deal of faith and trust in these people, as they should. I think they’re just not aware—they’re not aware of the challenges and the lack of funding and the way the system is sort of precariously balanced on top of volunteer hours to an incredible amount. I think the future in my mind, if you look at the data and volunteerism trending down, it’s trending down across all sectors, but that is hitting EMS very hard.
If you look at staffing, we’re seeing with low unemployment that means that it’s harder and harder to fill positions. That especially happens in rural areas. People are moving to urban areas for jobs. There’s not as many people there. If they do still live in the rural area, they tend to work in a neighboring larger town or other towns, so it’s harder for them to volunteer. So I just think the data is pretty clear where we’re headed. We just culturally have to try and do some heavy lifting and change the perceptions of what a society should pay for. As Dana Sechler from the Professional Ambulance Association of Wisconsin often says, we pay for garbage collection at $138, the median per capita cost per year. Like I said, some [areas are paying just] $12 per year for EMS. Garbage is very important. I don’t mean to dismiss it, but I think we can do better for lifesavers. I see that as the primary issue.
Garbage is very important. I don’t mean to dismiss it, but I think we can do better for lifesavers. I see that as kind of the primary issue. I think another issue is certainly something we’re hearing that is in rural areas, you have a lot of Emergency Medical Responders (EMRs). They’re taking a class that is 80 hours [in duration] because they want to help their neighbors. They’re not transporting— they are showing up to be of help. But they’re taking the National Registry tests in Wisconsin, and the National Registry tests, for a lot of good reasons, is lifting the industry into a level of professionalism and knowledge that is important and necessary. But I think that certainly what we heard is that an EMR is sort of an entry level to this.
So how can we figure out a way to lower the barriers to participation, without lowering the standards of care? That’s something we need to look at. And I think frankly, as a nation, we need to look at that and have that conversation with the National Registry. I think they’re doing the work that they do, and, and in a lot of ways it’s good work, but I think they need to have feedback from their customers and all of us states are their customers. All of us need to maintain a dialogue with them and say, this is what we need. We may need critical thinking in our clinicians, but do we need it in our technicians? Do we need it in our EMRs? [For EMRs] do we need sort of tricky questions that two of them are correct and you have to sort of guess which correct answer you wanted to give? I think it’s that sort of stuff that demoralizes local people who may not be eager to take a test in the first place and are a little put off by a computerized test in the second place. Then if they don’t pass, they go right back home to their church, their gas station, and their bar and tell everybody how this impossible test is not worth their time. I’m not against the National Registry tests, but I do think that we need to have more conversation about it and we need to find ways to lower the barriers and maybe that’s preparing EMRs in a different way.
I’ve got a daughter who is preparing for the ACT [college entrance test], and she’s learning the tips and tricks. She’s in a class just to help her take that test, and a lot of it’s not even about the content. Maybe since the National Registry is modeled on these other types of tests we need to train more on not necessarily the skill levels of how to save someone’s life, but how to take a test, which seems a little weird. But if that is our standard, then we need to make sure that our people are prepared when they walk into that room.
Amanda Riordan: That makes a lot of sense. Certainly we hear feedback in both directions from a variety of different stakeholders regarding the increasing professionalization of EMS. On one end, of course, we want to honor and maintain the contributions of those mission critical volunteer providers, particularly in rural areas, and on the other hand we have the push-pull of a Paramedic, in particular, looking for additional certifications and additional recognition of mobile health care as a profession. All of that mixed together with a flat or diminishing reimbursement makes sustaining a mobile healthcare/EMS in all areas really challenging. But of course as you so aptly pointed out, it especially impactful areas of our country and in a state like Wisconsin where you have so much land mass that is in rural areas. [These issues] particularly impact states of that nature is as they look forward to an aging population and the movement of younger people into urban areas. So truly appreciate those insights and those suggestions. And it’s certainly something that I’m sure there will be continued dialogue about for years to come.
John Eich: And I would like to say that I see a real difference between a Paramedic—or in Wisconsin, we also have the Advanced EMT classification—where we are expecting them to have a body of knowledge and to be healthcare clinicians, to be making life or death decisions in the field. Absolutely. Everyone in society wants those people to be the best-trained, the most knowledgeable, at the top of their game. And the tests should reflect that. I do think that if we have someone who is a firefighter who’s driving out to a site to assist, that’s not the same as a Paramedic and I’m not saying that they shouldn’t be trained and there shouldn’t be a gates for them to go through. We need to be sure that they are trained to the best of their scope and to the best of their ability. But I think it’s a different level of care is a different kind of professionalism. So I think we just need to really make sure that we’re doing a service to the rural areas where they are scraping together five people to cover a very large area and they just don’t have time for the level of nuance that you will often see in an urban, metro area where you’ve got, um, you’ve got enough staff to cover these sort of things,
Amanda Riordan: Makes complete sense and certainly something that we know so many communities are wrestling with right now. I thank you for bringing it to everyone’s attention. I think that we will get some lively dialogue in the comments when we get this posted about, as you pointed out, the diminishing volunteerism as well as the other pressures facing most mobile healthcare these days. Before we wrap up here, would you mind giving us some tips or thoughts about how EMS providers, mobile healthcare providers, in Wisconsin can work best with your office? Or if you have any generalized tips about how ambulance services and fire departments across the country can best work with the Offices of Rural Health in their state, we would be very grateful. Clearly you are moving and shaking in Wisconsin and we’d love to see that ripple out to other states.
John Eich: Absolutely. So, I have counterparts in every state and they’re all doing great work when it comes to rural health and rural EMS. If someone in any state simply goes to Google and, enters their state name and “office of rural health,” they’ll get right to them. I think there is a difference between Offices of Rural Health. Many of us are in state government, and so what you experienced there is common of state government—It’s a more bureaucratic system. The websites tend to be a little bit trickier to find the information because there’s obviously a lot going on there and some political considerations. We [here in Wisconsin] are university-based. There’s about 12 of those around the nation, and three that are nonprofit, so, even leaner and more flexible. So every [office] will look differently.
I do think that EMS should reach out to their Offices of Rural Health to let them know about their needs, because when we look at metrics for healthcare and for population health, we see the metrics getting worse. It’s almost like a horseshoe in that they get worse the more rural and remote you are. Suburban areas have the lowest need, and then the inner city tends to be equally challenging. We share a lot of population health issues with inner cities. The difference I think is really transportation. We’re farther away. And if you don’t have a car, you’re really isolated and stuck, so EMS is mission critical.
If you think about that first hour of care being so important to outcomes, [if sick or injured in a rural area] your first half hour could be without care as people are getting to you and you’re trying to find a cell signal to actually call 911. Once they arrive, your rural EMS providers are the people that are giving you that care. So it is vitally important that those people have the resources to do their job the best that they can.
Please reach out to express your needs. One of the things we’ve been talking about based on this Rural Listening Tour and talking with our state EMS office and the associations just yesterday is the idea of some kind of helpline; Somebody to answer the call when a service is identifying that they are really struggling, because [rural services] are a little nervous about calling the state and saying, “Hey, guess what? Things are really rough here. You might want to shut us down.” Nobody wants that. The state EMS office is very clear that it’s not in anybody’s best interest to remove care and burden neighboring services. So getting a helpline with a number of resources and even someone that can drive out and sit across the table and talk through some issues and get some advice would be very helpful for some of these services that are really struggling. Those are some ways that I think folks can get involved, and I’m always interested in hearing more.
Amanda Riordan: John, thank you so very much for your time and insights today. It has been an absolute pleasure talking to you and I’m sure that we’ll be hearing a lot more from the Office of Rural Health, you, and your staff in the years to come. So again, we truly appreciate it and wish you a very happy National Rural Health Day tomorrow, November 15th.
John Eich: Thank you very much, and I look forward to celebrations around the nation.
Empathy is about trying to understand, as best we can, someone else’s situation or experience. The question is, do we in EMS truly understand the word? Are we empathetical to ourselves and to the people we work with?
While some say that empathy comes from proper upbringing, today’s decline in civility means we see less and less of it displayed. A major contributing factor is the “tough” exterior we favor in each other: how often have you heard comments like “come on, just suck it up buttercup,” “you need to be tougher than that to be a medic,” or “we’re EMS, we eat our young.” Why are we like this, and why can’t we reinforce the empathy that naturally resides in all of us?
Empathy is a big part of our jobs, and we need to teach it to our students, our employees and each other. People need to feel that it’s OK to be empathetic and that it’s a natural part of the whole EMS picture.
One of the best techniques to foster empathy is active listening — not only to our patients but also to staff and co-workers. When you actively listen, you H.E.A.R. …
Halt: Stop whatever else you are doing, end your internal dialogue on other thoughts, and free your mind to give the speaker your attention.
Engage: Focus on the speaker. We suggest a physical component, such as turning your head slightly so that your right ear is toward the speaker as a reminder to be engaged solely in listening.
Anticipate: By looking forward to what the speaker has to say, you are acknowledging that you will likely learn something new and interesting, which will enhance your motivation to listen.
Replay: Think about what the speaker is saying. Analyze and paraphrase it in your mind or in discussion with the speaker and other classmates. Replaying and dialoguing the information you have heard will aid in understanding what the speaker is attempting to convey.”1
So always look at the other’s point of view and try to understand what he or she is facing. It just might change your attitude and make you a better provider.
Your EMS Reputation Depends on Three Cs—Credentials, Courtesy, Community
In EMS, your reputation is critical. Your character moves with you from provider to provider and from squad to squad; EMS is a small world where people know about you before you even step foot in the door.
People react to you based on judgments from not only real life, but also your digital life. With Facebook, Snapchat, Instagram and other social media networks so prevalent today, your social media profile serves as the basis of your reputation both professionally and privately.
Unfortunately, social media blunders abound among EMS providers, affecting their reputations and their future hiring ability. You can find hundreds of examples doing a quick online search; here are just two.
Three South Carolina responders fired for making statements like “idiots shutting down I-126. Better not be there when I get off work …” (Kaplan, 2016, para. 3)
A Brockton, Mass. dispatcher who said of a pregnant overdose patient, “She needs to be left to rot …” (Shephard, 2018, para. 5)
A better way to think of your reputation is the “Three Cs” — Credentials, Courtesy and Community.
Credentials may also be called Continuing Education, as it’s vital to keep learning throughout your career. Many of the best paramedics and EMTs are lifelong learners; in contrast there are others who take the NREMT exam and then never do more to see EMS from a wider perspective.
Courtesy means being courteous not only to your patients and coworkers but also to yourself. When others feel comfortable around you, it is easier to develop those close ties and professional relationships that boost your reputation.
Community refers to both where you live and the broader EMS community at large. The public and our industry look to us to build and improve a framework where we can all grow and thrive. Professional norms promote collaboration, knowledge sharing and a collective responsibility for improving ourselves and our treatments.
So, let’s follow the “Three Cs” to improve EMS as a community. Let’s have better, more convenient education that goes beyond the “same old, same old.” Let’s push our medical directors for improved, evidence-based treatments. Let’s pull each other up and be leaders at the healthcare table. Lastly, let’s stand out in the community with reputations that reflect the consummate professionals we truly are.
Scott F. McConnellis Vice President of EMS Education for OnCourse Learning and one of the Founders of Distance CME, which recently launched a new learning platform. Since its inception in 2010, more than 10,000 learners worldwide have relied on Distance CME to recertify their credentials. Scott is a true believer in sharing not only his perspectives and experiences but also those of other providers in educational settings
When we think of trafficking, we generally think of drugs or weapons, not human beings. Yet the problem exists in numerous communities where EMS responders deliver care.
Human trafficking is defined by the United Nations as “the recruitment, transportation, transfer, harboring, or receipt of persons by improper means for an improper purpose.” (End Slavery Now, 2018, para. 1) A more succinct definition comes from Kathryn Brinsfield, MD, MPH, Assistant Secretary for Health Affairs and Chief Medical Officer for the Department of Homeland Security: “Human trafficking is modern-day slavery.” (DHS, 2017, para. 3)
Why is this so important in today’s EMS field? We are the first on scene, we are the ones invited inside where others are not and we are the ones who see an injured person’s environment. Our interactions with others can help us spot some of the tell-tale indicators.
Unfortunately, there are many reasons people are trafficked:
Domestic Slavery: People are brought into private homes to work as slave labor, with no options to leave.
Sex Trafficking: Children, men and women are forced into the commercial sex industry
Forced and Bonded Labor: People are forced to work under the threat of violence for no pay — often to repay a debt — without the ability to leave
Forced Marriage: Women and children are forced to marry another against their will and without their consent.
As an industry, there is much that EMS can do. We must keep our ears and eyes open, and report things that raise red flags in our minds. Some of the most common indicators we will see as emergency responders are:
Signs of abuse, wounds or bruising in various stages of healing or malnutrition
Scars or mutilations, including tattoos showing ownership
Language or cultural barriers preventing injured persons from communicating with you
Submissive or nervous appearances
Security measures like overly hardened doors or windows preventing movement of people
DHS has a great educational sheet with additional indicators to look for: click here for a printable copy. While a particular situation may turn out not to be what you suspect, report your suspicions regardless so trained law enforcement experts can evaluate the situation. Your hunch may save a life or multiple lives. Call Immigration and Customs Enforcement at 1-866-DHS-2-ICE (1-866-347-2423) or online here. You can also receive additional training here.
EMS has always been the forefront of medicine, delivering care to the sick and injured in various roles dating as far back as the Civil War. It has come a long way from the days of horse and buggy. Yet, where are we going now?
One look at the trajectory of Nursing indicates where we are headed. When Nursing first started, the profession was comprised of caring women who were viewed and treated as indentured servants, subservient to the male dominated physicians. Nursing evolved when the “servant” became educated. What followed were thousands of women beginning to diagnose, conduct research and improve outcomes in the healthcare field. Soon thereafter, they broke free of the care assistant model they were in. I see EMS following the same path.
The ambulance industry started out as transporters, with a curriculum that was adopted and funded by the Department of Transportation (DOT). The industry has roots in DOT, Police Departments, Fire Departments and the military, but are truly physician extenders that should be firmly rooted in Health Departments. EMS is now developing a language, doing research, obtaining national accreditation for our schools, even supporting continuing education with CAPCE. But we need to do more.
Outreach will help accomplish what many have started. We need to consider the picture the public has of EMS, especially when we have overlooked self-promotion for decades.
Let’s be the ones who show the public what EMS is and is capable of. I look forward to EMS education mirroring, “The Georgia Trauma Commission,” which collaborated with the Georgia Society of the American College of Surgeons and the Georgia Committee on Trauma to create the “Stop the Bleed” campaign. This inspiring crusade is designed to train school teachers, nurses and staff across the state on how to render immediate and potentially life-saving medical aid to injured students and co-workers while waiting for professional responders to arrive.” (2018, para. 4) This type of training gives us face time with the public so they can learn what we do and what we do not.
One of the other important outreach programs to help us in this endeavor is the Community Paramedic Program. We are seeing this education transform EMS into new and exciting roles in the community. “First responders frequently respond to calls for social services. So, the emergency responders may know of people who need some sort of services or resources,” (Todd) Babbitt, a former fire chief, said. “This team could help connect those people with the services they need. It’s about getting everybody to work together and communicate.” (2018, para. 4)
What we can do is start to get EMS in front of the public. Teach. And open our historically closed doors to the folks that make it easier to do our jobs. Educate others and learn together how our roles are changing modern day healthcare while embracing the change. Otherwise we risk being left in the dust by our progressive healthcare brethren.
References
(2018, Feb 1st, 2018). Ga. School Nurses Train to Stop the Bleed. The Brunswick News. Retrieved from https://www.emsworld.com/news/219782/ga-school-nurses-train-stop-bleed
(Ed.). (2018, January 30th, 2018). Conn. Fire Chiefs to Form Community Action Team. Norwich Bulletin. Retrieved from https://www.emsworld.com/news/219757/conn-fire-chiefs-form-community-action-team
There has been a lot of talk recently in social media and the news about leaving Narcan behind after a reversal of an opioid overdose. A new voluntary program in Pittsburgh, PA allows the state to pay for Narcan atomizers that EMS can leave with friends and family of OD patients. The media buzz revolves around the idea that we are enabling this cycle of addiction; “There is some pushback that maybe you’re enabling the problem a little bit, but at least in the short term, reduce the chances that person is going to die and you create more opportunities to get them into treatment,” said Mark Pinchalk, patient care coordinator for Pittsburgh EMS.” (Media, 2018, para. 3) I agree with Mr. Pinchalk that as an EMS Provider we are not there to judge, we are there to render aid.
One of my early instructors said, “Scott, your purpose is to leave the patient better than the way you found them.” I have taken that long ago statement to heart ever since, trying to leave the patient better than the way I found them whether that is medically as in a Diabetic whose blood glucose I raise from 20mg/dl to 130mg/dl or the person who receives a ride to the hospital to be checked out. EMS is about providing care. When we use our own judgements or opinions on our patients, it impedes or influences the care we provide.
These particular cases seem to bring out strong opinions surrounding a delicate issue. Thousands of people die every year from Opioid overdoses. A healthy percentage of them get their start on prescription pain killers. So where do we help? How do we not judge going to the same address three or four times a week to treat the same person in the same situation? These are just some of the tough questions providers and services face every day in America. Although we are trying to hold back the tide with a broom, it is up to us to provide the same level of care each and every time, regardless of the person or situation.
Will leaving Narcan at the scene save lives? Yes, I believe so. Will it encourage more drug use? I can’t be sure. Time will tell.
In comparison, studies show making birth control available to teens actually reduces sexual activity and reported pregnancies. Consider 2017 data that shows “Among adolescent females aged 15 to 19, 42 percent report having sex at least once. For males, that number was 44 percent. The numbers have gradually dropped since 1988, when 51 percent of female and 60 percent of male teens reported having had sex.” (Welch, 2017, para. 4)
So for now, I encourage the opportunity, as the law allows, to provide Narcan, knowing it doesn’t make the problem go away. And I look forward to EMS impacting this youthful epidemic. How? Community Paramedicine are the resource to embrace. Just like any other frequent patient, community paramedics will help those get the services they need including the much-needed follow up care.
Scott F. McConnell is Vice President of EMS Education for OnCourse Learning and one of the Founders of Distance CME, which recently launched a new learning platform. Since its inception in 2010, more than 10,000 learners worldwide have relied on Distance CME to recertify their credentials. Scott is a true believer in sharing not only his perspectives and experiences but also those of other providers in educational settings.
Mark Postma, AAA President & Asbel Montes, AAA Payment Reform Chair
The recent merger of Aetna/CVS may be the catalyst that finally brings the change that the ambulance industry has been advocating for over the past several years. This new healthcare strategy supports the ambulance industry’s ideas that alternative patient destinations are needed in EMS.
To explain this better, one must understand the current state of ambulance reimbursement via the 911 system or equivalent. At this point in time most commercial payers of healthcare (Insurance) as well as Medicare will not pay for 911 ambulance transportation to any destination other than the “nearest appropriate” hospital based emergency room; arguably, the most expensive and least efficient form of healthcare. The continuation of this policy discounts the advanced capabilities of both EMS and new clinical settings and the savings that can be achieved through innovative change. In addition, at the same time that the cost of healthcare in general is increasing, reimbursement from all payers is decreasing, creating a significant challenge for providers. Medicare consistently pays providers below cost for providing life-saving services and state Medicaid agencies are consistently underfunding the critical services to the un- and under-insured populations that have allowed intermediaries to delay or not pay ambulance services.
Much of the U.S. population believes that vital 911 EMS services or the equivalent are provided free or included in their local property taxes. This is generally not the case. While EMS services must be at the ready on a 24/7/365 basis, they are not paid for being on call, but only when the service is used.
Many communities have governing rules that require 911, or the equivalent, paramedic services to arrive on-scene within 8-12 minutes of receiving the call. This cost of readiness is VERY expensive. Skyrocketing personnel costs, ambulances, equipment, and other high cost drugs only exacerbate an already fragile reimbursement structure. Although recent articles about calling Uber or Lyft sound intriguing, these drivers and cars are not prepared for any type of injury. Nor can they alert the hospital in critical situations to have the heart cath lab ready or a trauma surgeon on standby, shortening the time to definitive care when time matters most. Emergency paramedics are highly trained, are nationally and/or state certified, and provide services on state regulated ambulances equipped to manage all types of emergencies. Ambulances are also often strategically placed to arrive in that 8-12 minute response time requirement. However, there is one piece missing from the ambulance scenario that allows for Uber/Lyft to succeed; your personal credit card is on file with them. NO GUARANTEED PAYMENT, NO TRANSPORT. The cost of providing ambulance services “on call” with life-saving equipment, medications, and personnel at the ready is steep. When you consider the many regulations providers must adhere to outside of patient care, the cost increases even more. This misunderstanding of the cost often results in patients being stunned when they receive a bill for services provided and feel that it is excessive. However, comparing the cost of a life-saving ambulance transport to an Uber/Lyft ride is like comparing the cost of building a house to putting up a tent.
On the other hand, these highly trained paramedics, with vehicles that are comprehensively (medically) equipped to meet the highest safety standards, have no credit card on file. They do not treat you based on your ability to pay. In fact, approximately less than half of ambulance patients have insurance, and when commercial insurance does pay, they are increasingly paying only a percentage of the total bill, leaving their insured left to pay the balance. In a time of an emergency, insurers should not place an additional burden on their insured through underpayment or claiming out of network status. In addition, although many emergency 911 calls begin as a “frantic call for help,” not all are life threatening and require the highest level of care; however, they do need some type of a health care intervention.
It is this high volume of low acuity patients who do not have primary care physicians and who currently by law must be transported to hospitals that continue to bottleneck emergency rooms. This bottleneck then requires ambulances to be “on the wall” at local hospital emergency rooms. The cost to the 911 EMS system rapidly begins a domino effect where all the patients begin to be diverted/directed to other hospitals causing an overflow to the next hospital. In large EMS systems, this domino effect can bring emergency rooms at all available hospitals to capacity quickly. EMS units are unable to go on additional emergency calls because they are caring for a patient while waiting on hospital staff to become available to take over. They also cannot leave that hospital with the patient to go to another hospital due to federal laws that prohibit this movement.
So why does the AETNA/CVS excite the leaders of EMS organizations? Most people assume that since this acquisition just occurred, Walgreens will probably follow suit with another insurer. Other local pharmacy “CVS types” may partner with local hospitals or medical insurance cooperatives as well. This leads the ambulance industry to believe that the capacity to transport patients to alternative locations could greatly change the landscape of EMS. The idea that local CVS/Walgreens/clinics could receive low acuity patients breaks open the bottleneck and can provide several benefits for the ambulance service and patient. One benefit is that adding these stores/clinics greatly increases the resources for caring for low acuity patients and could potentially double the locations an ambulance can transport to, which will allow for quicker transport times and increase efficiencies. Lastly, and most importantly, diverting the low acuity patients to these additional community resources would reduce overflow in the emergency departments and allow true emergency patients to be transferred over more quickly to receive the higher level of care they require. This scenario is also a win for the patient. They could be transported to the most appropriate location to care for their needs and therefore can be billed more accurately for services they require rather than the emergency department fees which are usually costlier.
To make this happen, obviously the CVS system needs to evolve to receive these patients. More importantly, ambulance reimbursement by federal, state, and private payers must evolve to meet the demands of the market. Due to the complexities of how EMS services are provided because of state and local regulations, mandatory response times, service area parameters, and others, reimbursement for these services must be adequately paid for by Medicare, Medicaid, and private insurers. Today EMS agencies can only “hope” that their patients have a source of payment!
Although one would think that this state of concern for EMS services is being monitored, it currently has only a very small voice in the healthcare continuum. Federal agencies seem to want to look at what EMS will look like in 10 to 25 years rather than where EMS is today and where it can develop over the next few years. EMS reform needs to happen soon to save these systems from bankruptcy and/or the public from higher taxation.
We hope that this merger will be the beginning of alternative EMS/ambulance destinations with allocated reimbursements that meet the costs of providing high quality, efficient, and necessary 911 ambulance services.
Mark Postma, COO, Sunstar Paramedics
American Ambulance Association, President
Works for Sunstar Paramedics, Florida’s largest EMS provider
MPostma@sunstarems.com, 727-224-0295
Asbel Montes, Vice President, Acadian Ambulance Service, Inc.
American Ambulance Association, Chair-Payment Reform Committee
Works for Acadian Ambulance Service, Inc., Louisiana’s largest EMS provider
Asbel.Montes@acadian.com, 337-291-3310
When discussing this new and growing field of pre-hospital care, there seems to be two unique paths that services are following. The first is the hospital-owned or contracted service, where community providers seek ways to decrease readmission rates for CHF, COPD, Pneumonia, Sepsis, MI and other chronic illnesses.
When a patient discharged with one of these targeted conditions is readmitted within a 30 day window, “hospitals face penalties of up to 3 percent of Medicare payments in 2018” (Gluck, 2017, para. 10). That is a lot of money. Consider, “Lee Health, Southwest Florida’s largest hospital operator, which is expected to lose $3.4 million in payments” (Gluck, 2017, para. 2). This model represents the if, or, and type of service, meaning if we can do it for less and there are providers willing to do this type of medicine, then we can save the expensive penalties from CMC.
The other model of community paramedicine is 911 abuse reduction. For years EMS has conditioned the public to call 911 for any emergency. But today, what we consider an emergency is far from the public’s perception of an emergency. “EMS has experienced a 37% increase in 911 calls since 2008.” (White, 2016, para. 6) Yet have we increased staffing proportionally to meet the demand? Afraid not since “only 50% of EMS services in 2008 were fully staffed, and more than 63% had a volunteer component as part of their staffing level” (“Critical Staffing Shortages,” 2015, para. 2).
The article references increasing wages to help compensate for the decrease in trained providers by attracting more professionals to the field. With the CMC limiting payments and the major insurance companies following suit, doubtful this will be an option in the near future.
To reduce calls and increase levels of service, we can try to reeducate the public to what is a true emergency, but that is a long and slow process. For example, Philadelphia has started the trend and placed several billboards up around neighborhoods that contribute an ordinarily high amount of non-emergent 911 calls. Will this work? Time will tell but I would believe not enough to affect the volume of calls.
What about enlisting Community Paramedics in these situations? I believe this is a viable solution with nurses triaging the low acuity calls in the 911 center. Dispatching Community Paramedics armed with not only the usual equipment, but also the knowledge base to connect these patients with primary care physicians, social workers, and the programs that are available to them. This will help people receive the long-term care they deserve.
Scott F. McConnell is Vice President of EMS Education for OnCourse Learning and one of the Founders of Distance CME. Since its inception in 2010, more than 10,000 learners worldwide have relied on Distance CME to recertify their credentials. Scott is a true believer in sharing not only his perspectives and experiences but also those of other providers in educational settings.
Fentanyl is a powerful drug that can be 50 times more potent than heroin. First responders are being warned to take precautions to avoid being exposed to the drug. Photo courtesy of the Drug Enforcement Administration.
The explosion of the opioid epidemic that is responsible for thousands of overdoses and deaths is a consistent problem that EMS and law enforcement encounter on an almost daily basis. Usually, the victims of these powerful drugs, such as heroin and fentanyl, are opioid users, who EMS personnel and law enforcement are regularly called to assist. However, first responders are also being warned about the increased risks they face of being exposed to these deadly drugs, specifically fentanyl—a popular synthetic opioid that is 40 to 50 times more powerful than heroin. To respond to these dangers, the Drug Enforcement Administration (DEA) released a field guide called “Fentanyl: A Brief Guide for First Responders” for EMS and police who find themselves responding to opioid-related calls.
“We need everybody in the United States to understand how dangerous this is,” Acting DEA Administrator Chuck Rosenberg warned. “Exposure to an amount equivalent to a few grains of sand can kill you.”
The warnings have become more urgent in recent months due to numerous cases of accidental overdoses and exposures involving EMS and police.
In May, Chris Green, a police officer with the East Liverpool Police Department, was accidentally exposed to fentanyl during a routine traffic stop after he inadvertently ingested the drug through his skin. Green needed four shots of Narcan, an emergency overdose medication, to be revived after collapsing from the effects of the drug. In another case, two Paramedics and a sheriff’s deputy in Hardford County, Maryland, were treated after showing signs of opioid exposure while treating an overdose victim.
“It is important to get the word out to everyone because it may be the first responder who needs to have Narcan administered,” said Baltimore City Health Commissioner Leana Wen.
The risks of accidental exposure are so high, in fact, that some emergency personnel have even begun carrying Narcan kits for drug-sniffing K-9s, just in case the dogs ingest the deadly drugs.
The DEA guide, along with a National Institute for Occupational Safety and Health manual on preventing fentanyl exposure, suggests certain precautions be taken to lower the risk of coming in direct contact with the substance. Personnel should be able to recognize the signs and symptoms of an overdose, be aware of the ways fentanyl can be ingested, and only allow trained professionals to handle substances that are suspect.
“Assume the worst,” Rosenberg said. “Don’t touch this stuff or the wrappings that it comes in without the proper personal protective equipment.”
Each year, the American Ambulance Association honors best practices, ingenuity, and innovation from EMS providers across the country with our AMBY Awards.
Gold Cross Ambulance’s Documentation Project Project Awarded a 2016 AMBY for Best Quality Improvement Program
The documentation review process at Gold Cross Ambulance had not changed much since the day of paper trip tickets. Retrospective documentation feedback was being given to crews, but they were not fully utilizing the capabilities of their technology to analyze the feedback and make significant improvements. Gold Cross Ambulance hypothesized that improved documentation goals would lead to better patient care and increased reimbursements. They knew they needed to make improvements in the review process and to better utilize the technology that was already in place. In addition to the documentation goals, they identified the opportunity to work some small, but significant, clinical improvements into a documentation project. One initial focus of clinical improvement was making sure the field crews were obtaining at least two sets of vital signs on every patient, and properly documenting these vital signs in the electronic patient care report (ePCR). Of all the performance indicators we measure, trending of vital signs touches every patient contacted. Educators from Utah EMS for Children shared research citing “inadequate recognition of and response to hypotension and hypoxia was associated with higher odds of disability and death” (Hewes H., 2016). This was such a basic thing to measure, but it had potential to impact every contacted patient. Gold Cross know that vital signs were an area in which they could improve, while also meeting their documentation goals. To do so, they implemented the following:
Create a way to measure overall documentation quality.
Establish a formal standard for documentation and educate crews about the documentation expectations.
Improve the overall documentation of the ePCR.
Improve the number of patients with properly collected and documented vital signs.
Improve amount of reimbursement and decrease collection cycle time.
Gold Cross formed a work group to tackle these issues, which consisted of members of the Quality Department, Training Department, Billing Department, and Operations Department. The group meets every other week to evaluate progress and assess the need for adjustments to the system. Mid-year of 2014, the group worked to revise the program for documentation evaluation. A new standard was created based on the ePCR fields. A point system was established for documentation which gave each ePCR field a weighted number of points, equaling 100%. Incomplete or missing fields result in a loss of points for that field, which provided a way to measure documentation performance. The scoring data is tracked in our ePCR quality module, allowing us to analyze and report on the data easily. The feedback on any areas of missed points is sent to the crew via the ePCR messaging system, so it is easily accessible to the crews during regular daily tasks. Feedback is focused on improvement comments instead of punitive comments. Positive feedback is included in each evaluation. The group released an initial version of the General Instructions for the ePCR, which was an internal manual detailing expectations for every field in our ePCR. The focus was to provide clear expectations to all field crews regarding how to properly fill out the ePCR and what content should be included. The training department created an educational program on the online educational software program, detailing the documentation guidelines and testing the crews on the material. The General Instructions for the ePCR were also posted on the company training site, so crews would have easy access at any time. The Quality Department developed a class for the newly hired providers. The class emphasizes the need for quality documentation, outlines the program, and includes actual documentation examples for evaluation and discussion. Patient advocacy through documentation is instilled in the participants of this class. The Billing Department developed a class which is taught at six months after hire. In the class, documentation is reviewed from class participants. The billing department shows how the bill is processed from the documentation, and they discuss common challenges to the billing process. The program has been monitored with continuous PDSA cycles and has been adjusted as needed for continued improvement.
An initial company goal for documentation was set at 90%. From project start to current date, the company-wide documentation averages have increase from 74% at the beginning of the project to 96% currently. Field crews have expressed greater clarity in the company expectations for documentation. The overall average documentation scores by division are posted regularly for the company to view, and this has had the additional benefit of sparking a competitive streak between some of our divisions, further improving the scores. The improvement in collection of vital signs not only improved overall patient care, but resulted in a Performance Improvement Award from the Utah State Bureau of EMS in 2016. The bureau looked at pediatric vital signs and recognized two rural and two urban EMS agencies in the state for their improvements. Gold Cross Eastern Division won the award for a rural agency, and Gold Cross Salt Lake Division won for the urban agency. Their study found our agency improved the collection of pediatric vital signs by 53% in our urban area and 66% in our rural area.
The most important impact of this project is improvement in patient care, which is our primary mission. The goals for complete documentation have encouraged field crews to make sure they complete proper assessments, since they know those areas of the ePCR are evaluated and must be complete. Improvements in assessment result in better differential diagnoses and improved treatment plans and outcomes. The documentation project has positively impacted Gold Cross financially as expected. Reimbursement rates have increased and the time to complete the collection cycle has improved. Due to the documentation improvements, the billing staff spends less time researching information, following up on incomplete documentation, and fighting in appeals.
Congratulations to Gold Cross Ambulance for the Reduced Readmissions Project’s selection as a 2016 AMBY Winner for Best Community Impact Program.
The American Ambulance Association is sad to report that Barry M. Mogil, former CAAS reviewer and director of communications for Pinellas County, Florida EMS, passed away.
Our thoughts are with his family. Barry’s contributions to Florida EMS will not be forgotten.
The Special Needs Tracking & Awareness Response System (STARS), was founded just over two years ago at SSM Health Cardinal Glennon’s Children’s Hospital in St. Louis, Missouri. The team at Cardinal Glennon realized that they needed to do something to address the growing number of children in the U.S. with special health care needs, many of whom are at a higher risk for repeated ambulance transports.
As an EMT for over 18 years, Patricia Casey, the Missouri Coordinator of the STARS Program, knows how intimidating it can be for a first responder to walk into a home that in many ways may look like a hospital room. Children with special health care needs can require many different types of in home medical equipment that first responders are often not familiar with. The STARS Program aims to make the job of the first responders easier while making children with medical needs and their parents more comfortable with ambulances in case they need to be transported in one.
Cardinal Glennon works with local ambulance districts to enroll children with special medical needs in that district’s STAR Program. Once a child is registered in STARS, they are given a unique patient identification number and a home visit is scheduled with the patient and their family to compile pertinent medical history. Participating ambulance companies then create a book with all of the stars in their area so that their first responders have access to the medical information on the go. If a STAR needs to be transported, their caregiver can relay their STAR number to the dispatcher who will then let the first responders know. First responders can then look up crucial medical information about the STARS patient, so they can be better prepared when they arrive on scene.
Knowing that many medical devices in the homes of the STARS may be foreign to first responders, Cardinal Glennon’s staff provides free necessary trainings all around Missouri and now Illinois. Shelby Cox works as the Team Lead for EMS outreach, and Josh Dugal, RN, is the EMT-P STARS Coordinator for Illinois. Together with Casey, they help keep the program running smoothly. Each participating ambulance company appoints a STARS coordinator on their staff who will make biannual home visits and make sure the STARS medical information is up to date. Cardinal Glennon also sets up regular opportunities for STARS to visit their local first responders. Giving STARS the chance to get familiar with an ambulance and their local first responders prior to a medical emergency has been proven to help out both parties when an emergency occurs.
A paramedic who has responded to STARS calls explains that “the STARS system permitted me to have advanced medical knowledge before I walked through the door. There was no time lost backtracking to learn the patient’s history or baseline in the midst of a chaotic scene”. In addition to helping the first responders, the STARS program has been a huge reassurance to the parents of STARS whose children may often need medical assistance.
To learn more about Cardinal Glennon’s STARS program, visit their website or check them out on Facebook. Also check out Patricia Casey’s Article on the STARS Program which includes testimonials from both parents and first responders who have participated in the program.
Thanks to the entire team at Cardinal Glennon for your great work!
Do you know of other innovative programs being run by ambulance services? Share with the AAA so that we might feature those programs on the AAA Blog as well.
Last week, American Ambulance Association staff took a road trip south to tour the Richmond Ambulance Authority. Known across the country and around the world for their innovative approach to EMS, RAA certainly did not disappoint.
Thank you to Chip Decker, Rob Lawrence, Dan Fellows, Elizabeth Papelino, Danny Garrison, Dempsey Whit, Jason Roach, and the whole RAA team for the hospitality and generosity with their time!
By Desiree LaFont, Education & Events Director, American Ambulance Association
October 2015
In a previous life I worked for a hospitality-related association. Within that industry there was something known as the “Gaylord Effect”—when Gaylord Hotels would open a property in a city, all of the other businesses in the area, including other hotel brands, benefitted. High standards, a sterling reputation, and the ultimate in customer service meant Gaylord booked convention and leisure business on a scale few could rival. Everyone from the local cab drivers to the bartenders to the surrounding hotels profited from the huge influx of travelers. Where once feared as the luxury brand that would crush the competition, they were soon seen as a desirable ally. So fast forward a few years, and I have a new life working for the American Ambulance Association (AAA), but I often think about the Gaylord brand and their ability to change a city with their commitment to their customers. If you are wondering what any of this has to do with ambulance services, I’m about to get to that.
On a recent trip to Louisiana to document the tenth anniversary of Hurricane Katrina and the role AAA members had in the recovery, the AAA’s Director of Membership, Amanda Riordan, and I had the opportunity to visit Acadian Ambulance. Armed with a local videographer, a short list of questions, and a crippling doubt in our ability to capture what is arguably the most important private EMS story in recent history, we arrived at Acadian’s Air Med Station in Lafayette, Louisiana.
Lafayette Headquarters
Our first interview was with Marc Creswell, Acadian’s Air Med Operations Manager. Marc’s story is incredible for a number of reasons, and I won’t attempt to retell all of it here, but I will tell you Marc is the kind of guy that could have inspired the phrase, “when the going gets tough, the tough get going.” This is the guy you want in your foxhole. And to be honest, we could have completed our interview with Marc, packed up, and had more than enough material to tell a great story about Acadian and Katrina, but Acadian was just getting started.
We spent the remainder of the day interviewing Dee Dee Sewell, their Critical Support Intervention Specialist; Clay Henry, Acadian’s Vice President of Operations, Communications Center; Blane Comeaux, President of Acadian Total Security; and Chairman and CEO Richard Zuschlag. Everyone, including Mr. Zuschlag, gave us more time then we could have hoped for and held nothing back. They shared a great many operational details, but always through the lens of the story of the people behind all those unseen efforts and rescues.
Downtown New Orleans
Dee Dee at work in Lafayette
The next day we visited downtown New Orleans to meet with Steven Kuiper, Regional Vice President for Acadian. Within minutes, I felt like I was hearing the story of Katrina for the first time. Steven shared facts, but, once again, it was wrapped in the story of the people around him—the suffering and the heroism he personally observed on the ground.
And, then came the big finish; Janie Fuller, Paramedic Field Supervisor and lifelong resident of St. Bernard Parish. Janie accompanied us to the Mayor’s Office to interview Deputy Mayor Andy Kopplin and New Orleans Director of EMS Dr. Jeffrey Elder. She then gave us the insiders’ tour of her parish and showed us exactly where the levees were breached. Her entire hometown was under eighteen feet of water in 15 minutes, but by nightfall Janie had commandeered an airboat and was taking a cardiac patient to I-10 and Causeway for evacuation. Needless to say, Janie is a force of nature herself, and no matter what dark alley a call takes her down, this lady is coming out alive and so is her patient.
Telling the Story
[quote_right]What also emerged during our visit was Acadian’s ability to tell the human side of what it means to be in EMS. They tell the Katrina story and the story of their company with humility, grace, and a deep appreciation for their colleagues and the many other services that stepped in to lend a hand.[/quote_right]What emerged over the course of those two days of interviews was the amazing story of what Acadian, and private EMS, were able to accomplish in the midst of the hurricane’s devastation. Hospitals were shuttered, law enforcement was overrun, citizens were cut off, and conditions for everyone—including EMS—were unspeakable. Despite this, medics in the area stayed and other ambulance services rolled in.
Hundreds of ambulances with trained medics rolled in to help New Orleans and countless communities throughout Louisiana, Mississippi and Alabama. Whether or not they knew how bad the situation was, they still went in. No one can ever calculate what that response meant to the City of New Orleans and the other affected areas, but I think we all have a sense of how much worse it would have been without the timely response of private EMS. What also emerged during our visit was Acadian’s ability to tell the human side of what it means to be in EMS. They tell the Katrina story and the story of their company with humility, grace, and a deep appreciation for their colleagues and the many other services that stepped in to lend a hand.
So after an incredible 48 hours in Louisiana we had to head home, and I left with a heavy heart. I wanted to stay a little longer. No, I wanted to stay a lot longer. But why? As I sat on the plane home, it hit me. It was the Acadian Effect. Acadian is that big, shining example of what an innovative, self-determined private EMS company can mean to the population they serve. How you can put people first and come out a winner. How when you put people first everyone benefits. Telling the incredible Acadian success story benefits all of EMS because it typifies the EMS culture of going beyond what’s required and how maintaining human dignity is an essential part of patient care.
So let’s tell that story! Let’s tell the story of Acadian and Katrina. Let’s tell the story of Sandy, Joplin, the Boston Bombing, and the thousands of times a day private EMS responds to 9-1-1 with compassion and highly skilled medical knowledge because that’s your chosen profession. Let’s tell the story until the press, the public and the legislators are telling it for us.
Our heartfelt thanks to Acadian and every AAA member we have the privilege of serving.
Want More?
Watch AAA’s Katrina & Rita retrospective video that features many of the subjects of this blog post.
Founded in 1971 in with just eight staff and two vehicles, Acadian Ambulance has grown over the years to more than 4000 employees with a fleet of 400 ground ambulances, helicopters, fixed-wing airplanes, and van and bus transports. Their territory has expanded from Lafayette Parish, Louisiana, to stations spanning large swaths of Louisiana, Texas, and Mississippi.
How does such a large and varied service feed their talent pipeline? In addition to many other strategies, Acadian is leading the industry in its efforts to engage young adults in EMS through its High School Champions program, a division of their National EMS Academy.
Porter Taylor, Acadian’s Director of Operations
To learn more about the ins-and-outs of the program, AAA caught up with Porter Taylor, Acadian’s Director of Operations. Taylor has been in EMS for 29 years, since he joined Acadian Ambulance as a college sophomore. “I love making a difference in people’s lives. When I was working on a unit it was the patient, and now, almost 30 years later, it is the employees that I love helping.”
Establishing High School Champions was not a linear path. Initially, Acadian would send medics to career fairs and school functions to introduce the field and promote its National EMS Academy (NEMSA) as an opportunity after graduation. “There are a lot of technical grants out there, and a critical staffing need for EMS in general. We wanted to create an avenue for educating students about the benefits of becoming EMTs to support our staffing needs long term,” said Taylor.
Although these medic visits were effective, Acadian wanted to expand the fledgling program’s scope and reach. He began visiting area high schools and meeting with school boards and directors more than a year ago to build relationships and explore opportunities. The partnerships he built added another facet to the High School Champion initiative wherein Acadian continues to promote NEMSA, coupled with an effort to get the schools to incorporate an EMT program as an elective prior to graduation. “[I wanted] to introduce them to our company and our support of this technical career path. My goal was to let the teachers and technical program directors know that Acadian has jobs for their students upon the successful completion of the program. Once students turn 18, Acadian will be able to offer them a rewarding position with good pay and benefits and with continuing education opportunities.”
Acadian Operations Manager Justin Cox was instrumental in the implementation at Livonia High School, a recent addition to the program. In concert with his professional know-how, Cox had a personal connection to the school—his thirteen year old daughter attends Livonia.
Collaborating with the administration, Acadian now works with schools like Livonia to introduce EMS career paths at the end of high school, a time when students are making key choices about their futures. Students can start the EMT training program as an elective prior to graduation and take the national certification exam upon turning 18. Students spend 2-3 hours 3 days a week, during their junior and senior years preparing. “It is a joy to work on this program,” said Taylor, “It is a privilege to help young people make a career choice that is full of rewards.”
Does your service have a great program that is making a difference in your area? Let us know in the comments section below, or email ariordan@ambulance.org.
As we approach the ten year anniversary of Hurricanes Katrina and Rita, AAA is working to gather the stories of the many members who rallied to assist in these crises.
Do you have a memory, photo, or video you would like to share with the ambulance service community? If so, please complete the brief form below, and we will add your story to our retrospective.
All content contributors will be entered into a raffle for a free registration to AAA’s 2016 Stars of Life.
Ambulance services interact with people from all walks of life, and from all parts of the world. AAA checked in with expert Marcia Carteret, M.Ed., for some tips for communicating more effectively with people from other cultures. Marcia is an instructor of intercultural communications at University of Colorado School of Medicine in the Department of Pediatrics. She trains residents, faculty, and staff in healthcare communication with a focus on cross-cultural patient care and low health literacy. She has also trained in over 120 private pediatric and family practices across Colorado.
In all healthcare settings, successful communication with patients and families depends on awareness of three key barriers to their understanding and compliance:
Cultural Barriers: Understanding western medicine and the U.S. healthcare system is a challenge for many of us, but it is especially problematic for recent immigrants and refugees. 72% of U. S. population growth in the next 20 years will come from immigrants, or the children of immigrants.
Limited English Proficiency: The number of people who spoke a language other than English at home grew by 38 percent in the 1980s and by 47 percent in the 1990s. While the population aged 5 and over grew by one-fourth from 1980 to 2000, the number who spoke a language other than English at home more than doubled.
Low Health Literacy: While poor understanding of the health care system and difficulty understanding health care instructions may be associated with language and cultural barriers, low health literacy is also found in patients who are proficient in English and who share the common U.S. culture. This latter group may be especially at risk of having their low health literacy go unrecognized. 90 million “mainstream” Americans cannot understand basic health information.
Addressing These Barriers
How do people understand one another when they do not share a common cultural experience? Nowhere is this a more pressing question than in healthcare settings, especially in emergencies. There is no easy list of things “to do” or “not to do” that can be applied to each culture. What can be useful are communication guidelines that work for people from all cultures. These guidelines are also important for people with low health literacy.
[quote_left]“The essence of cross-cultural communication has more to do with releasing responses than sending messages. And it is most important to release the right responses.” — Edward T. Hall[/quote_left]
Perhaps the most important is framing questions to elicit appropriate answers. As Edward T. Hall, anthropologist and cross-cultural researcher wrote,“The essence of cross-cultural communication has more to do with releasing responses than sending messages. And it is most important to release the right responses.” What could be more crucial when, for example, an EMT or paramedic is attempting to establish level of consciousness by directly eliciting information from a patient? Being able to get quality responses from patients from any culture is a communication skill that comes with experience. Learning and practicing a set of strategically designed questions is key to building confidence in this important skill.
Key Communication Tips
Explain your professional role 911 is the number to dial in an emergency, but some people may not understand the roles of different emergency responders. You can’t expect people who are still learning to function in the U.S. mainstream society – recent immigrants or refugees especially – to understand the role of the EMT or paramedic.
Suggested explanation: “I am not a doctor. I am an emergency medical professional. I have come to help because someone called 911. I will take this person who is hurt/sick to the hospital safely.”
Use simple familiar words and short sentences “Stabilize” is a complex word, even though it might be the best word to describe what you do for a patient in an emergency. Help is a better word. With Limited English Proficiency (LEP) patients and families, the 5¢ word is always better than the 75¢ word. Basics such as give, take, more, less will be better choices than administer, increase, decrease.
Be clear when you are asking a question versus giving an instruction. Running questions and statements together is confusing for second language learners. Avoid sentences like this: “It looks like you are having a reaction (a statement of observation) so I need to know if you have taken any medication that made you feel sick.”Examples of concise phrasing:
“What medicine have you taken?
“Show me this medicine.”
“Show me where it hurts.”
Avoid close-ended questions These usually begin with do, did, does, is, are, will, or can. These can be answered with a simple yes or no – or a head nod. Avoid the use of close-ended questions with Limited English Proficiency (LEP) patients because in many cultures people will frequently simply say yes even if they don’t understand you.
Use open-ended questions These usually begin with the 5 Ws – who, what, when, where, why (and how or how many). It is awkward to answer these questions with a nod, shrug, or simple yes/no. For example, you might ask: “When did you take these pills?” instead of “Did you take these pills?”
Avoid starting sentences with negations such as isn’t and didn’t. Though this is a common speech pattern in English, it may be confusing for people who speak a different native tongue. For example: Didn’t you call 911? (Read more about this speech pattern.)
Clarify understanding – yours and theirs Even if you are using simpler words and shorter sentences, you can’t be certain there has been communication until the receiver acknowledges it with feedback. Remember, head nodding does not count as feedback with people from many different cultures. Even with Americans, and definitely with children, head nodding is often a sign of partial comprehension. So you must ask clarifying questions.
Repeat back what you have understood.
Examples: “Yes? – you took the medicine?”
“Yes? – you are his/her grandmother?”
Not understanding vs. misunderstanding When people do not understand what you say, there is more likely to be an indication of confusion than when they MISunderstand you. A person struggling with English, for example, may ask you to repeat what you have said. Their face may show confusion. But when people MISunderstand, it can be far less obvious. For example, the English words want and won’t sound very much alike to a non-native speaker. You may say to a person, “I want to help you,” but she may hear “I won’t help you.” She may be perplexed that this is your response, but she may be very inclined to accept the word of a healthcare professional. She may perceive you as being uncaring, but certainly won’t say so. Many MISunderstandings go unnoticed by both parties. Asking clarifying questions is crucial.
Speak slowly and clearly—NOT loudly Often when people don’t understand our language, we treat them as if they are hearing impaired or “slow” without realizing we are doing so. Articulate your words in shorter phrases rather than just speaking more loudly.
Cultural Norms
Cultural norms vary around the world. Here are some key norms to keep in mind when assisting patients and their families.
Eye Contact
An EMT or Paramedic will often be perceived as an authority figure by the people from more traditional cultures. If a person is avoiding eye contact while listening to you or while answering questions, be aware that in some cultures direct eye contact with an authority figure is very rude. In trying to be respectful, people may appear to be avoiding looking you in the eye. This is not to be taken immediately as any indication of disrespect, dishonesty, or evasiveness
Silence Silence may be the only response a person can muster if he or she is frightened. Silence might also be a way of showing respect, similar to avoiding eye contact. Being thoughtful about answering a question shows humility and real effort in giving the best answer. Unfortunately, silence on the part of the non-English patient or family member is often interpreted as open hostility by Americans. It can be helpful to say: “I need your help. Please try to answer my questions. Your answers help me help you.” Also, try not to rush answers. Americans allow very little time between questions and responses. Impatient and in a hurry we tend to start talking before the other person is able to answer the question asked.
Reverting to Native Language Bilingual patients may revert to their language of origin in times of stress, and while this hinders communication with an EMT, it should not be seen as manipulative or uncooperative. Calmly ask the person, “Can you speak in English? Please try English.” If the person does not speak any English, this will at least help them realize you can’t understand.
Summary
As first-responders, EMS is often working in high stakes situations where communication is a challenge even without the added barriers associated with the “triple threat” to healthcare communication—language barriers, cultural understanding, and low health literacy. No matter which culture an EMT or Paramedic is interacting with, the key to good communication is asking good questions and phrasing all dialogue in simple short sentences. It should be clear that a question is being asked or a statement of information is being made by the EMS professional. Asking for clarification is essential. Head nods and affirmative answers should not be accepted immediately as evidence of sufficient understanding or agreement. EMTs will find that enhanced communication skills will not only improve cross-cultural interactions, these skills improve outcomes with all people – even “mainstream” Americans. Also, be aware that low health literacy is a problem for 90 million Americans. Never assume that same-culture communication in English requires less intentional speech on your part.





 In honor of today’s
In honor of today’s 

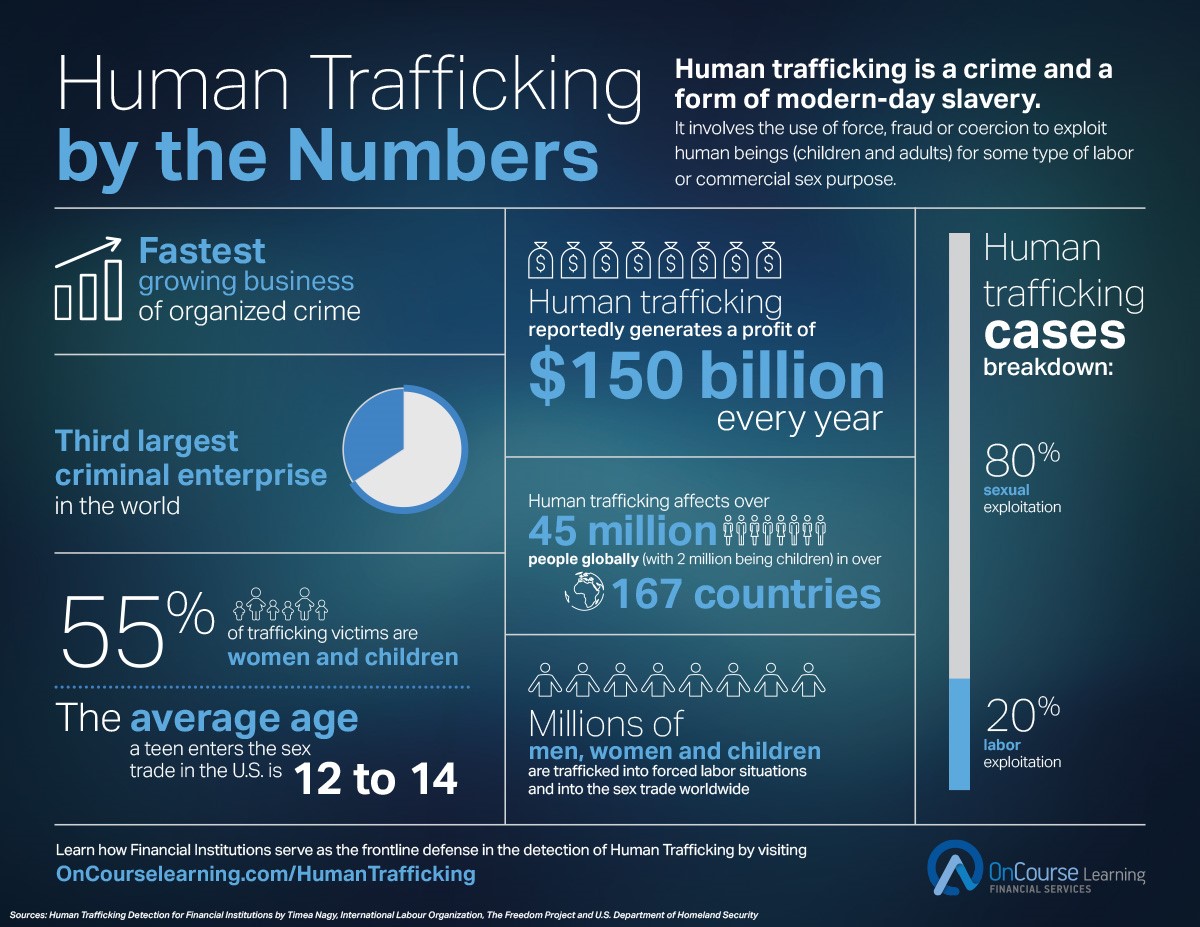


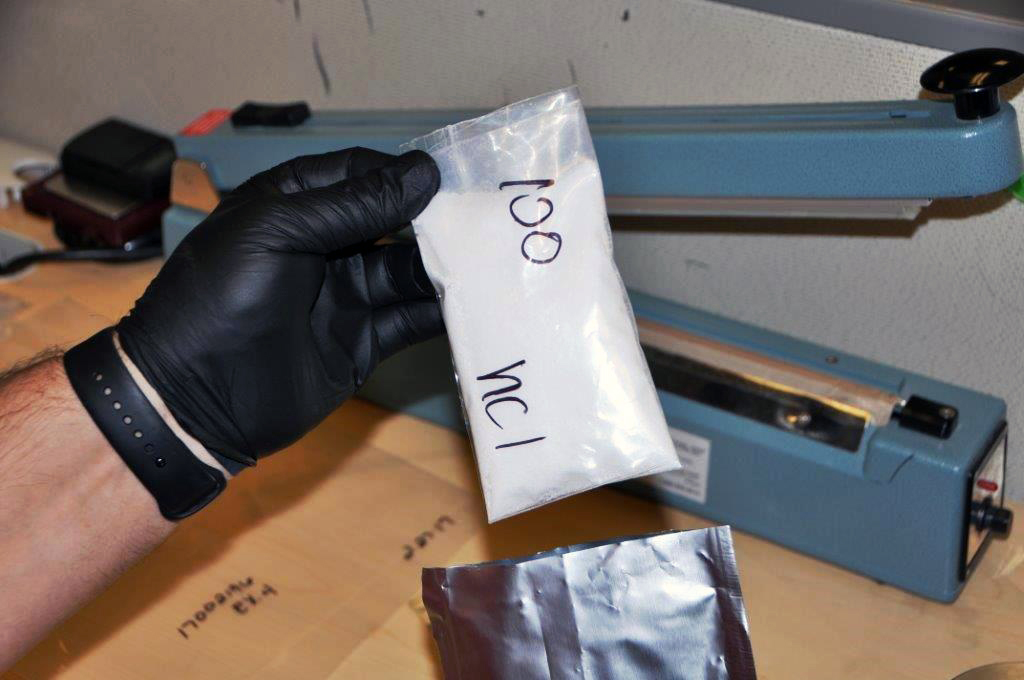

 The documentation review process at Gold Cross Ambulance had not changed much since the day of paper trip tickets. Retrospective documentation feedback was being given to crews, but they were not fully utilizing the capabilities of their technology to analyze the feedback and make significant improvements. Gold Cross Ambulance hypothesized that improved documentation goals would lead to better patient care and increased reimbursements. They knew they needed to make improvements in the review process and to better utilize the technology that was already in place. In addition to the documentation goals, they identified the opportunity to work some small, but significant, clinical improvements into a documentation project. One initial focus of clinical improvement was making sure the field crews were obtaining at least two sets of vital signs on every patient, and properly documenting these vital signs in the electronic patient care report (ePCR). Of all the performance indicators we measure, trending of vital signs touches every patient contacted. Educators from Utah EMS for Children shared research citing “inadequate recognition of and response to hypotension and hypoxia was associated with higher odds of disability and death” (Hewes H., 2016). This was such a basic thing to measure, but it had potential to impact every contacted patient. Gold Cross know that vital signs were an area in which they could improve, while also meeting their documentation goals. To do so, they implemented the following:
The documentation review process at Gold Cross Ambulance had not changed much since the day of paper trip tickets. Retrospective documentation feedback was being given to crews, but they were not fully utilizing the capabilities of their technology to analyze the feedback and make significant improvements. Gold Cross Ambulance hypothesized that improved documentation goals would lead to better patient care and increased reimbursements. They knew they needed to make improvements in the review process and to better utilize the technology that was already in place. In addition to the documentation goals, they identified the opportunity to work some small, but significant, clinical improvements into a documentation project. One initial focus of clinical improvement was making sure the field crews were obtaining at least two sets of vital signs on every patient, and properly documenting these vital signs in the electronic patient care report (ePCR). Of all the performance indicators we measure, trending of vital signs touches every patient contacted. Educators from Utah EMS for Children shared research citing “inadequate recognition of and response to hypotension and hypoxia was associated with higher odds of disability and death” (Hewes H., 2016). This was such a basic thing to measure, but it had potential to impact every contacted patient. Gold Cross know that vital signs were an area in which they could improve, while also meeting their documentation goals. To do so, they implemented the following:


 Our first interview was with Marc Creswell, Acadian’s Air Med Operations Manager. Marc’s story is incredible for a number of reasons, and I won’t attempt to retell all of it here, but I will tell you Marc is the kind of guy that could have inspired the phrase, “when the going gets tough, the tough get going.” This is the guy you want in your foxhole. And to be honest, we could have completed our interview with Marc, packed up, and had more than enough material to tell a great story about Acadian and Katrina, but Acadian was just getting started.
Our first interview was with Marc Creswell, Acadian’s Air Med Operations Manager. Marc’s story is incredible for a number of reasons, and I won’t attempt to retell all of it here, but I will tell you Marc is the kind of guy that could have inspired the phrase, “when the going gets tough, the tough get going.” This is the guy you want in your foxhole. And to be honest, we could have completed our interview with Marc, packed up, and had more than enough material to tell a great story about Acadian and Katrina, but Acadian was just getting started.



