
NEMSAC Meeting November 1–2
|

|
|
|
|
|
|
|

|
|
|
|

Please either or Join!

 |
|
|
Today, the Centers for Medicare & Medicaid Services (CMS) released the latest enrollment figures for Medicare, Medicaid, and the Children’s Health Insurance Program (CHIP). These programs serve as key connectors to care for more millions of Americans. Medicare As of May 2022, 64,553,288 people are enrolled in Medicare. This is an increase of 103,837 since the last report. 34,893,853 are enrolled in Original Medicare. 29,659,435 enrolled in Medicare Advantage or other health plans. This includes enrollment in Medicare Advantage plans with and without prescription drug coverage. 50,086,253 are enrolled in Medicare Part D. This includes enrollment in stand-alone prescription drug plans as well as Medicare Advantage plans that offer prescription drug coverage. About 12 million individuals are dually eligible for Medicare and Medicaid, so are counted in the enrollment figures for both programs. Detailed enrollment data can be viewed here: https://data.cms.gov/summary- Medicaid and Children’s Health Insurance Program (CHIP) As of May 2022, 88,978,791 of people are enrolled in Medicaid and CHIP. This is an increase of 677,711 since the last report. 81,904,569 are enrolled in Medicaid 7,074,222 are enrolled in CHIP For more information on Medicaid/CHIP enrollment, including enrollment trends, visit https://www.medicaid.gov/ Every day, CMS ensures that people across the U.S. have coverage that works. See the latest coverage totals across all CMS programs at https://www.cms.gov/pillar/ |

 |
| The next CMS Ambulance Open Door Forum scheduled for:
Date: Thursday, August 18, 2022 Start Time: 2:00pm-3:00pm PM Eastern Time (ET); Please dial-in at least 15 minutes before call start time. Conference Leaders: Jill Darling, Maria Durham **This Agenda is Subject to Change**
Chair- Maria Durham, Director, Division of Data Analysis and Market Based Pricing Moderator – Jill Darling (Office of Communications)
Slide presentation is available at: https://www.cms.gov/Center/ 2. CY 2023 Hospital Outpatient Prospective Payment System (OPPS) and Ambulatory Surgical Center (ASC) Payment System Proposed Rule: https://www.federalregister. Proposals Regarding Rural Emergency Hospitals Ambulance Services III. Open Q&A **DATE IS SUBJECT TO CHANGE** Next Ambulance Open Door Forum: TBA ODF email: AMBULANCEODF@cms.hhs.gov —————————— This Open Door Forum is open to everyone, but if you are a member of the Press, you may listen in but please refrain from asking questions during the Q & A portion of the call. If you have inquiries, please contact CMS at Press@cms.hhs.gov. Thank you. Open Door Participation Instructions: This call will be Conference Call Only. To participate by phone: Dial: 1-888-455-1397 & Reference Conference Passcode: 5109694 Persons participating by phone do not need to RSVP. TTY Communications Relay Services are available for the Hearing Impaired. For TTY services dial 7-1-1 or 1-800-855-2880. A Relay Communications Assistant will help. Instant Replay: 1- 866-469-7806; Conference Passcode: No Passcode needed Instant Replay is an audio recording of this call that can be accessed by dialing 1-866-469-7806 and entering the Conference Passcode beginning 1 hours after the call has ended. The recording is available until August 20, 2022, 11:59PM ET. For ODF schedule updates and E-Mailing List registration, visit our website at http://www.cms.gov/ Were you unable to attend the recent Ambulance ODF call? We encourage you to visit our CMS Podcasts and Transcript webpage where you can listen and view the most recent Ambulance ODF call. The audio and transcript will be posted to: https://www.cms.gov/Outreach- CMS provides free auxiliary aids and services including information in accessible formats. Click here for more information. This will point partners to our CMS.gov version of the “Accessibility & Nondiscrimination notice” page. Thank you. |

|
|
|
|
|
|
|

Please either or Join!

|
| |

|
|
|
|
|
|
SAMHSA anticipates 988 will continue to grow and evolve over the years. In 2021, the Lifeline received 3.6 million calls, chats, and texts. That number is expected to at least double within the first full year after the 988 transition.
SAMHSA continues to hold convenings with state, territorial, and tribal leaders – as well as crisis contact centers, public safety answering points, and behavioral health providers – to prepare for 988. One of the most urgent needs involves staffing at crisis centers. Anyone interested in serving in these critical positions is encouraged to visit the 988 jobs web page. |
|
|
Connect With Us     |
|

Please either or Join!

2022 SESSION
Wednesday, June 8, 2022 1:00 p.m. – 3:45 p.m. Virtual Meeting Washington, DC
General Meeting1:00-1:05 Welcome, Introductions, Opening Remarks Jonathan Greene, Deputy Asst. Secretary for Preparedness & Response Director, Office of Emergency Management & Medical Operations FICEMS Chairperson Gam Wijetunge, Director, NHTSA OEMS Director of the Office of EMS, NHTSA Elizabeth Fudge Supervisory Program Analyst, Health Readiness Policy & Oversight Theresa “Tee” Morrison-Quinata EMS for Children Branch Chief, Maternal & Child Health Bureau Division of Child, Adolescent, & Family Health 1:20 Assistant Secretary for Preparedness & Response Jonathan Greene Deputy Assistant Secretary & Director, Office of Emergency Management & Medical Operations
1:25 Indian Health Services Darrell LaRoche Director, Office of Clinical & Preventive Services
1:30 Centers for Disease Control & Prevention Christine “Chris” Kosmos Director, Division of State & Local Readiness Center for Emergency Preparedness & Response
1:35 Centers for Medicare & Medicaid Services CAPT. Skip Payne Director, Emergency Preparedness & Response Operations 1:40 Countering Weapons of Mass Destruction Office Pritesh Gandhi, M.D. Chief Medical Officer, EMS Program
1:45 United States Fire Administration Richard Patrick Director, National Fire Programs Directorate 1:50 National Highway Traffic Safety Administration Nanda Srinivasan Associate Administrator, Research & Program Development 1:55 Public Safety & Homeland Security Bureau David Furth, J.D. Deputy Chief, Office of the Bureau Chief 2:00 State EMS Directors Update Steve McCoy EMS Bureau Florida Department of Public Health Kate Elkins EMS Specialist, NHTSA OEMS 2:10 COVID-19 First Responder Deaths Dave Bryson EMS Specialist, NHTSA OEMS 2:15 National 911 Program Update Brian Tegtmeyer National 911 Program Coordinator 2:20 NEMSIS Update Eric Chaney EMS Specialist, NHTSA OEMS 2:25 National Roadway Safety Strategy – Post Crash Care Gam Wijetunge Director, NHTSA OEMS
Diane Pilkey, DHHS HRSA | Max Sevareid, NHTSA OEMS
2:35 EMS Data Standards & Exchange Subgroup Rachel Abbey, DHHS ONC | David Millstein, DHS USFA 2:40 EMS Systems Integration & Preparedness Subgroup Tee Morrison-Quinata, DHHS HRSA | Gam Wijetunge, NHTSA OEMS 2:45 Workforce & Safety Subgroup Greg Williams, DHS USFA | Dave Bryson, NHTSA OEMS 2:50 Education & Training Subgroup Michael Stern, DHS USFA | Clary Mole, NHTSA OEMS
3:25-3:30 Public Comment |
The National EMS Advisory Council (NEMSAC) will host a virtual meeting on Wednesday and Thursday, May 11-12, 2022. Members of the public can register for the webcast here.
The NEMSAC meets several times each year to discuss issues facing the EMS community. Members of NEMSAC provide counsel and recommendations regarding EMS to the National Highway Traffic Safety Administration (NHTSA) in the Department of Transportation (DOT) and the Federal Interagency Committee on EMS (FICEMS).
Daily agendas include time for NEMSAC subcommittee deliberations in the morning and the publicly webcasted portion of the meetings begin at 1:00 pm ET, Wednesday, May 11, 2022, and 12:00 pm ET on Thursday, May 12, 2022. Items on the agenda include:
Individuals registered for the meeting who wish to address the council during the public comment periods can review the current draft and interim advisories and submit comments in writing to NHTSA.NEMSAC@dot.gov by 5:00 pm ET on May 3, 2022.
Draft advisories:
Interim advisory:
This meeting will be open to the public. NHTSA is committed to providing equal access to this meeting for all program participants. Persons with disabilities in need of accommodation should send their request to Clary Mole by phone at (202) 868-3275 or by email at Clary.Mole@dot.gov no later than May 3, 2022. A sign language interpreter will be provided and closed captioning services will be provided for this meeting through the WebEx virtual meeting platform.
|
Notice of Public Meeting: This notice announces a meeting of the National Emergency Medical Services Advisory Council (NEMSAC).
In late April, CMS will issue a Comparative Billing Report (CBR) on Medicare Part B claims for ambulance ground transport. Use the data-driven report to compare your billing practices with those of peers in your state and across the nation.
CBRs aren’t publicly available. Look for an email from cbrpepper.noreply@religroupinc.com to access your report. Update your email address in the Provider Enrollment, Chain, and Ownership System to ensure delivery.
For More Information:

|

From ASPR on March 31, 2022
The National Advisory Committee on Seniors and Disasters (NACSD) and the National Advisory Committee on Individuals with Disabilities and Disasters (NACIDD) will soon host public meetings of these two advisory committees.
The next NACIDD meeting takes place on Friday, April 1 from 11:30 a.m. to 2:30 p.m. ET and the next NACSD meeting is on Wednesday, April 6 from 11:00 a.m. to 2:00 p.m. ET.
Join board members, distinguished guests, federal leaders, and other experts to discuss the challenges, opportunities, and priorities in meeting the unique health needs of older adult populations and people with disabilities during and after disasters and public health emergencies.
Advanced registration for these meetings is required and can be accessed, along with additional meeting agendas and public information, through the online event pages for the NACIDD and NACSD.
The agendas for each of the next meetings include time to hear from the public. The floor will be open to hear as many relevant comments as possible. To learn how to request a speaking time, please visit each committee’s event page. You can send questions about the NACSD to NACSD@hhs.gov and questions about the NACIDD to NACIDD@hhs.gov.

March 24, 2022
The Honorable Xavier Becerra
Secretary of Health and Human Services
Department of Health and Human Services
200 Independence Avenue, SW
Washington, DC 20201
Dear Secretary Becerra:
Ground ambulance service organizations and fire departments continue to struggle financially from the enduring economic effects of the COVID-19 public health emergency (PHE). Our respective members face sharp increases in the costs of fuel, equipment, medical supplies, and staffing as we deal with a severe shortage of paramedics and emergency medical technicians (EMTs) which has been an issue for years but exacerbated by the pandemic. We implore you to help ensure communities around the country have access to 9-1-1 emergency and non-emergency ground ambulance services through the remainder of the PHE and beyond with an infusion of $350 million from returned and/or unspent money in the Provider Relief Fund (PRF).
We greatly appreciate the funding that ground ambulance service organizations and fire departments have already received from the PRF. The funds have been a lifeline for many of our respective members and their ability to continue to serve their communities. However, as the Phase 4 distribution of funds demonstrated, more funding is needed for ground ambulance services. Our members indicate the funds they received in Phase 4 covered approximately 50% of their lost reimbursement and increased costs from July 1, 2020, to March 31, 2021, whereas previous distributions were closer to 88%. We therefore respectfully request an immediate distribution of $350 million or 10% of the annual Medicare expenditure on ground ambulance services.
We request that the funds be distributed in a similar manner as the Tranche 1 distribution from the PRF. The automatic, across-the-board deposit of funding was especially helpful for small and rural ground ambulance service organizations. These rural organizations provide care in underserved areas and are often daunted even by an abbreviated application process. To ensure equity for all communities, we support universal direct deposit.
Additionally, we encourage HHS to make these payments based on the National Provider Identification (NPI) number of the ground ambulance service organization or fire department rather than Tax ID Number (TIN). In the case of moderate and large cities, many municipal departments may share a TIN while maintaining distinct NPIs. Providing these payments according to TIN may unintentionally comingle funds intended for different departments such as fire departments, public health departments, and local government-run hospitals or clinics.
The American Ambulance Association (AAA), International Association of Fire Chiefs (IAFC), International Association of Fire Fighters (IAFF), National Association of Emergency Medical Technicians (NAEMT), and National Volunteer Fire Council (NVFC) represent the providers of vital emergency and non-emergency ground ambulance services and the paramedics, EMTs and firefighters who deliver the direct medical care and transport for every community across the United States.
Our members take on substantial risk every day to treat, transport, and test potential COVID-19 patients, and play a vital role in providing vaccinations to individuals in their homes. Ground ambulance service organizations and fire departments, however, urgently need the additional
$350 million to help offset the increased costs and lower reimbursement resulting from our vital response to the pandemic.
Thank you in advance for your consideration of this request.
Sincerely,
American Ambulance Association
International Association of Fire Chiefs
International Association of Fire Fighters
National Association of Emergency Medical Technicians
National Volunteer Fire Council

From NASEMSO on March 23, 2022
![]()
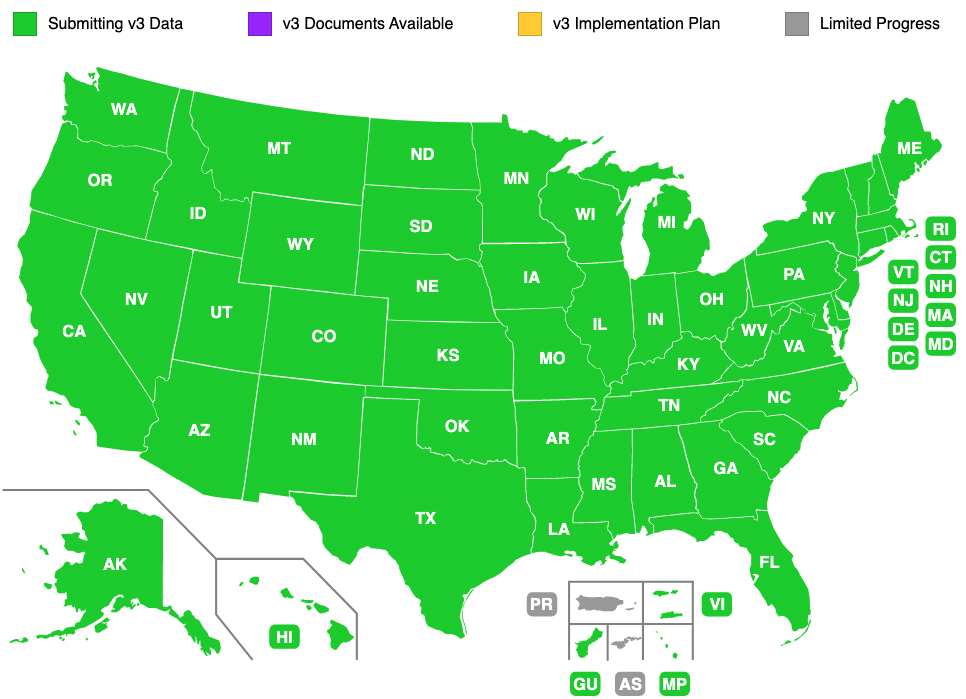
The National Model EMS Clinical Guidelines Project was first initiated by NASEMSO in 2012 and has produced three versions of model clinical guidelines for EMS: the first in 2014, a revision 2017, and now this third version in 2022. The guidelines were created as a resource to be used or adapted for use on a state, regional or local level to enhance prehospital patient care and can be viewed here. These model protocols are offered to any EMS entity that wishes to use them, in full or in part. The model guidelines project has been led by the NASEMSO Medical Directors Council in collaboration with six national EMS physician organizations, including: American College of Emergency Physicians (ACEP), National Association of EMS Physicians (NAEMSP), American Academy of Emergency Medicine (AAEM), American Academy of Pediatrics, Committee on Pediatric Emergency Medicine (AAP-COPEM), American College of Surgeons, Committee on Trauma (ACS-COT) and Air Medical Physician Association (AMPA). Co-Principal Investigators, Dr. Carol Cunningham and Dr. Richard Kamin, led the development of all three versions. Countless hours of review and edits are contributed by subject matter experts and EMS stakeholders who responded with comments and recommendations during the public comment period.
NASEMSO gratefully acknowledges the Technical Expert Panel, the Technical Reviewers, and many others who volunteered their time and talents to ensure the success of this project.
The comprehensive review and revision of these guidelines was made possible by funding support from the National Highway Traffic Safety Administration Office of EMS and the Health Resources and Services Administration Maternal and Child Health Bureau EMS for Children Program.
Andy Gienapp, MS, NRP
Deputy Executive Director
andy@nasemso.org

|
HHS Office of Intergovernmental and External Affairs COVID-19 Update for
March 21, 2022 |
|
|
|
|
|
Marvin B. Figueroa, Director
U.S. Department of Health and Human Services
Intergovernmental and External Affairs 200 Independence Ave., S.W. Washington, D.C. 20201 |
Connect With Us     |
From HHS Office of Inspector General on March 15, 2022
The COVID-19 pandemic created unprecedented challenges for how Medicare beneficiaries accessed health care. In response, the Department of Health and Human Services (HHS) and the Centers for Medicare & Medicaid Services (CMS) took a number of actions to temporarily expand access to telehealth for Medicare beneficiaries. CMS allowed beneficiaries to use telehealth for a wide range of services; it also allowed beneficiaries to use telehealth in different locations, including in urban areas and from the beneficiary’s home.
This data brief provides insight into the use of telehealth in both Medicare fee-for-service and Medicare Advantage during the first year of the COVID-19 pandemic, from March 2020 through February 2021. It is a companion to a report that examines the characteristics of beneficiaries who used telehealth during the pandemic. Another report in this series identifies program integrity concerns related to telehealth during the pandemic. Understanding the use of telehealth during the first year of the pandemic can shed light on how the temporary expansion of telehealth affected where and how beneficiaries accessed their health care. This information can help CMS, Congress, and other stakeholders make decisions about how telehealth can be best used to meet the needs of beneficiaries in the future.
We based this analysis on Medicare fee-for-service claims data and Medicare Advantage encounter data from March 1, 2020, to February 28, 2021, and from the prior year, March 1, 2019, to February 29, 2020. We used these data to determine the total number of services used via telehealth and in-person, as well as the types of services used. We also compared the number of services used via telehealth and in-person during the first year of the pandemic to those used in the prior year.
Over 28 million Medicare beneficiaries used telehealth during the first year of the pandemic. This was more than 2 in 5 Medicare beneficiaries. In total, beneficiaries used 88 times more telehealth services during the first year of the pandemic than they used in the prior year. Beneficiaries’ use of telehealth peaked in April 2020 and remained high through early 2021. Overall, beneficiaries used telehealth to receive 12 percent of their services during the first year of the pandemic. Beneficiaries most commonly used telehealth for office visits, which accounted for just under half of all telehealth services used during the first year of the pandemic. However, beneficiaries’ use of telehealth for behavioral health services stands out. Beneficiaries used telehealth for a larger share of their behavioral health services compared to their use of telehealth for other services. Specifically, beneficiaries used telehealth for 43 percent of behavioral health services, whereas they used telehealth for 13 percent of office visits.
Telehealth was critical for providing services to Medicare beneficiaries during the first year of the pandemic. Beneficiaries’ use of telehealth during the pandemic also demonstrates the long-term potential of telehealth to increase access to health care for beneficiaries. Further, it shows that beneficiaries particularly benefited from the ability to use telehealth for certain services, such as behavioral health services. These findings are important for CMS, Congress, and other stakeholders to take into account as they consider making changes to telehealth in Medicare. For example, CMS could use these findings to inform changes to the services that are allowed via telehealth on a permanent basis.

| HRSA eNews March 3, 2022 |
|
|
||||||||



 In his State of the Union address, President Biden announced an ambitious strategy to address our national mental health crisis. At the Health Resources and Services Administration, we stand with the President in his call for unity in our national response and know that for the millions of Americans living with a mental health condition or caring for a loved one with a mental health condition, the time for action is now.
In his State of the Union address, President Biden announced an ambitious strategy to address our national mental health crisis. At the Health Resources and Services Administration, we stand with the President in his call for unity in our national response and know that for the millions of Americans living with a mental health condition or caring for a loved one with a mental health condition, the time for action is now. In February, HRSA announced the winners of the Promoting Pediatric Primary Prevention Challenge, $66.5 million to support community-based vaccine outreach efforts, more than $560 million in pandemic relief payments to health care providers, funding to increase virtual care quality and access, and new funding to support primary care residency programs.
In February, HRSA announced the winners of the Promoting Pediatric Primary Prevention Challenge, $66.5 million to support community-based vaccine outreach efforts, more than $560 million in pandemic relief payments to health care providers, funding to increase virtual care quality and access, and new funding to support primary care residency programs.
 With this funding, nearly $19 billion will have been distributed from the Provider Relief Fund and the American Rescue Plan Rural provider funding since November 2021
With this funding, nearly $19 billion will have been distributed from the Provider Relief Fund and the American Rescue Plan Rural provider funding since November 2021
 Our
Our  A
A  Climate change influences human health and diseases in numerous ways. Underserved communities stand to bear the brunt of these climate-induced risks (e.g., extreme heat, poor air quality, flooding, extreme weather events). HRSA and CDC’s Climate and Health Program invite you to consider the impacts of climate change on the U.S. health care system. CDC will share its work to build resilience to these public health effects.
Climate change influences human health and diseases in numerous ways. Underserved communities stand to bear the brunt of these climate-induced risks (e.g., extreme heat, poor air quality, flooding, extreme weather events). HRSA and CDC’s Climate and Health Program invite you to consider the impacts of climate change on the U.S. health care system. CDC will share its work to build resilience to these public health effects.
 Children’s mental health continues to be a top priority for state leaders across both legislative and executive branches of state government. With COVID-19 exacerbating the challenges children are facing, there is much more work to be done.
Children’s mental health continues to be a top priority for state leaders across both legislative and executive branches of state government. With COVID-19 exacerbating the challenges children are facing, there is much more work to be done.
