The New England Journal of Medicine has rapidly published a peer-reviewed paper on the Snohomish County WA ‘Patient 1’. This was the first reported case of COVID 19 in the US. This seminal document, which given the magnitude of the case and its initial findings is released in full here
The work by Michelle L. Holshue, M.P.H., Chas DeBolt, M.P.H., Scott Lindquist, M.D., Kathy H. Lofy, et al for the Washington State 2019-nCoV Case Investigation Team was turned round in just over 5 weeks and below is an ‘Executive summary’ ( as extracted from the paper) but the full paper and range of results should be read in full.
Patient Presentation
On January 19, 2020, a 35-year-old man presented to an urgent care clinic in Snohomish County, Washington, with a 4-day history of cough and subjective fever. On checking into the clinic, the patient put on a mask in the waiting room. After waiting approximately 20 minutes, he was taken into an examination room and underwent evaluation by a provider. He disclosed that he had returned to Washington State on January 15 after traveling to visit family in Wuhan, China. The patient stated that he had seen a health alert from the U.S. Centers for Disease Control and Prevention (CDC) about the novel coronavirus outbreak in China and, because of his symptoms and recent travel, decided to see a health care provider.
On admission, the patient reported persistent dry cough and a 2-day history of nausea and vomiting; he reported that he had no shortness of breath or chest pain. Vital signs were within normal ranges. On physical examination, the patient was found to have dry mucous membranes. The remainder of the examination was generally unremarkable. After admission, the patient received supportive care, including 2 liters of normal saline and ondansetron for nausea.
Viral Presence
Both upper respiratory specimens obtained on illness day 7 remained positive for 2019-nCoV, including persistent high levels in a nasopharyngeal swab specimen (Ct values, 23 to 24).
Stool obtained on illness day 7 was also positive for 2019-nCoV (Ct values, 36 to 38).
Nasopharyngeal and oropharyngeal specimens obtained on illness days 11 and 12 showed a trend toward decreasing levels of virus
Day 8: Condition Improves
On hospital day 8 (illness day 12), the patient’s clinical condition improved. Supplemental oxygen was discontinued, and his oxygen saturation values improved to 94 to 96% while he was breathing ambient air. The previous bilateral lower-lobe rales were no longer present. His appetite improved, and he was asymptomatic aside from intermittent dry cough and rhinorrhea. As of January 30, 2020, the patient remains hospitalized. He is afebrile, and all symptoms have resolved with the exception of his cough, which is decreasing in severity.
History Taking
This case report highlights the importance of clinicians eliciting a recent history of travel or exposure to sick contacts in any patient presenting for medical care with acute illness symptoms, in order to ensure appropriate identification and prompt isolation of patients who may be at risk for 2019-nCoV infection and to help reduce further transmission. Finally, this report highlights the need to determine the full spectrum and natural history of clinical disease, pathogenesis, and duration of viral shedding associated with 2019-nCoV infection to inform clinical management and public health decision making.
Conclusion
There is little doubt that this paper is about to become a globally sited document as we continue to deal with COVID 19. As far as EMS and our first response to it goes, the paper reinforces the key actions currently being taken
Sample COVID-19 Policies for Mobile Healthcare Providers
Thank you to the following organizations for sharing their policies as examples.
Global Medical Response maintains a COVID-19 page to provide information to all members of the GMR community—clinicians and non-clinicians.
Updates from GMR Chief Medical Officer, Dr. Ed Racht
The intention of the COVID-19 Process/Policy Template is to provide agencies, medical directors, or others who want to utilize it, an outline/template on which to build an agency-specific policy/protocol to address COVID-19. This includes suggestions for development and/or oversight committees, outside partners and stakeholders, as well as preparation and process for EMS workers who provide best practice care for patients as well as providing for the protection of pre-hospital providers and medical director(s). Its application is totally up to the user.
This document is meant to be a living document that can be revised as circumstances or guidance changes. It can also be a discussion piece for those who choose to develop a different type of policy but may want to use some of the components of the document as a starting point.
President Donald Trump today signed H.R. H.R. 6074 into law, approving $8.3 billion in supplemental appropriations to fund programs in response to the COVID-19 illness. The bill would bolster vaccine development, research, equipment stockpiles, and state and local health budgets as government officials and health workers fight to contain the outbreak, which has claimed 11 lives in the U.S. and sickened more than 160 people across more than a dozen states.
The AAA advocated to negotiators of the bill that first responders needed to be included in the funding package and that all communities be eligible for the funding. Due in part to our outreach, the emergency funding provides a transfer of no less than $10 million to the National Institute of Environmental Health Sciences for worker-based training aimed at preventing exposure of the virus to emergency first responders, and others at risk of exposure (i.e., hospital employees).
The supplemental also appropriates $1 billion for state and local preparedness, which will allow state and local governments to carry out preparedness and response activities, with each State receiving a minimum of $4 million. Of the $1 billion, $300 million is allocated for global disease detection and emergency response, and FY 2019 Public Health Emergency Preparedness grantees.
The Centers for Medicare and Medicaid Services (CMMI) has released its initial list of applicants selected to participate in the ET3 pilot program. CMMI notes that the list is not final as it still needs to execute participation agreements with the applicants. CMMI will issue a final list once it completes the process.
Applicants from 36 states and the District of Columbia were selected to participate in the program. Approximately 200 applicants were approved with instances in which the same ambulance service organization submitted applications for multiple counties as well as more than one organization submitting an application for the same county. CMMI has sent notifications to each of the applicants letting them know to expect a follow up email with the partnership agreement, program guidance and additional details.
The ET3 program is a five-year voluntary pilot program designed to test the potential benefit to the Medicare program and patients of ambulance service providers and suppliers furnishing treatment in place as well as transport to alternative destinations. For more information about the ET3 program, please go the ET3 website.
On January 30, 2020, the Centers for Medicare and Medicaid Services (CMS) announced the roll-out of its “Healthy Adult Opportunity” (HAO) initiative. Under the initiative, participating states will have a portion of their current federal Medicaid funding converted to block grants. In return, the states will gain greater flexibility in providing for the health care needs of certain portions of their existing Medicaid populations.
In a letter directed to State Medicaid Directors, CMS outlined the details of how the HAO initiative would operate. The initiative will be operated under CMS’ 1115 waiver authority. In order to participate, a state must submit an application setting forth the specific demonstration projects it intends to implement. CMS reiterated that participation in the HAO initiative is voluntary. CMS further indicated that it will review state applications on a case-by-case basis and make an independent decision on whether the proposed policies merit approval. States with existing Section 1115 waivers that cover eligible populations will be permitted to transition existing demonstrations into the HAO initiative.
CMS indicated that HAO demonstrations will generally be approved for an initial 5-year period, and successful demonstrations may be renewed for a period of up to 10 years.
A summary of some of the major provisions of this initiative is provided below.
Federal Funding
The Medicaid Program is a joint federal and state program that provides free or low-cost health coverage to nearly 65 million Americans. The Program is administered by each state, with the federal government reimbursing states for a percentage of their qualifying Medicaid expenditures. The amount of federal matching funds is based on a statutory formula that compares a state’s per capita income to the national average. States with lower per capita incomes receive a higher Federal Medical Assistance Percentage (FMAP). FMAPs range from 50% to a maximum of 83%. In addition, the federal government provides higher matching rate (called an Enhanced FMAP) for certain services or populations. For example, the federal government currently pays 90% of the costs of providing health care to those covered by the Medicaid expansion included in the Affordable Care Act.
Under the HAO initiative, participating states would forego the FMAP for certain Medicaid populations. Instead, these states would receive a fixed amount of federal funding (i.e., a block-grant), which will be calculated based on either a total expenses or per-enrollee basis. To the extent the state spends more than its budgeted amount, it would not be eligible for additional federal matching funds. To the extent the state ends up spending less than its budgeted amount, the state would participate in the cost-savings.
Eligible Medicaid Populations
The HAO initiative is focused on the non-mandatory adult Medicaid populations, i.e., individuals that are under the age of 65, and who are not eligible for Medicaid on the basis of disability, or their need for long term care, and who are not otherwise eligible under a State Medicaid Plan. In other words, this initiative is largely targeted at those individuals that become eligible for Medicaid as a result of the Affordable Care Act.
Benefit Package Design
Under the HAO initiative, states will have the ability to design benefit packages that closely resemble the benefit packages provided by private insurers. At a minimum, this would include benefit packages that cover all of the Essential Health Benefits (EHBs) required for commercial insurances sold on the State ACA Exchanges. States may also design federally qualified health center coverages that facilitate the use of value-based payment design among safety-net providers.
Beneficiaries that are shifted into HAO demonstration projects will retain certain beneficiary protections, including all federal disability and civil rights laws, fair hearing rights, and limits on their mandatory cost-sharing amounts.
Coverage of Prescription Drugs
One major change would be to state’s coverage of prescription drugs. The initiative would give states the flexibility to offer formularies under an HAO demonstration project similar to those provided in commercial health insurance markets. This would remove the current mandate that states provide a so-called “open formulary.” States that elect to establish their own formulary would be required to comply with the EHB requirements regarding prescription drug benefits. States would also be required to cover substantially all drugs used to treat: (1) mental health disorders (i.e., antipsychotics and antidepressants), (2) HIV (i.e., antiretroviral drugs), and (3) opioid use disorders (i.e., all forms, formulations, and delivery mechanisms) where there are rebate agreements in place with the manufacturers.
In theory, this would permit states to cover only a single drug for many pharmaceutical classes.
Cost-Sharing Amounts
States would have the flexibility to impose additional cost-sharing obligations on beneficiaries covered under a demonstration program, subject to two broad limitations:
Aggregate out-of-pocket costs for beneficiaries covered under an HAO demonstration must not exceed 5% of the beneficiary’s household income, measured on a monthly or quarterly basis; and
Premiums and cost-sharing charges for tribal beneficiaries, those beneficiaries living with HIV, those beneficiaries needing treatment for substance use disorders, and the cost-sharing charges for prescription drugs used to treat mental health conditions must not exceed amounts permitted under the implementing regulations. States would also not be permitted to suspend enrollment for these individuals if they fail to pay their premiums or cost-sharing amounts.
Wrap-Around Services (Including NEMT)
States would be given the flexibility to discontinue the coverage of Alternative Benefit Plan wrap-around services, including non-emergency medical transportation (NEMT) and early and periodic screening, diagnostic and treatment services (EPSDT) for individuals aged 19-20.
On December 2, 2019, CMS posted the 2020 Ambulance Fee Schedule Public Use Files. These files contain the amounts that will be allowed by Medicare in calendar year 2020 for the various levels of ambulance service and mileage. These allowables reflect a 0.9% inflation adjustment over the 2018 rates.
The 2020 Ambulance Fee Schedule Public Use File can be downloaded from the CMS website by clicking here.
Unfortunately, CMS has elected in recent years to release its Public Use Files without state and payment locality headings. As a result, in order to look up the rates in your service area, you would need to know the CMS contract number assigned to your state. This is not something the typical ambulance service would necessarily have on hand. For this reason, the AAA has created a reformatted version of the CMS Medicare Ambulance Fee Schedule, which includes the state and payment locality headings. AAA members can access this reformatted fee schedule at the link below.
The proposed rule sets the foundation for the data collection system for ground ambulances. It proposes a stratified random sample method, that is very similar to the one the AAA proposed via the work we commissioned through The Moran Company. We are working through the stratification categories, which are slightly different than those we identified.
CMS also proposes the cost and revenue data elements it plans to use. There are some details in the proposed rule text and others will be in the proposed tool that will be posted the CMS website today.
CMS also proposes the collection period and penalties for failing to report.
While the data collection provision was the key component for ground ambulance services, CMS also proposed changes to the PCS requirement sought by the AAA. CMS is proposing to reference the PCS also as non-physician certification agreements. The agency is further proposing to clarify that the focus is on the certification of the medical necessity provisions and the form of the certification statement is not prescribed. As part of the non-physician statement, CMS is proposing expanding the staff of you may sign the statement when an attending physician is unable to sign.
Today, CMS has released the proposed rule that would establish the ambulance fee schedule cost collection system as required by statute. The AAA is currently reviewing the rule and will provide a more detailed summary in the coming days.
On Tueusday, July 30 at 12:00pm Eastern, the AAA will be hosting a free webinar during which AAA counsel will provide an overview of the proposals in the rule. Do not miss out on this chance for the most up to date information.
If you have questions about the legislation or regulatory initiatives being undertaken by the AAA, please do not hesitate to contact a member of the AAA Government Affairs Team.
Tristan North – Senior Vice President of Government Affairs tnorth@ambulance.org | (202) 802-9025
Ruth Hazdovac – AAA Senior Manager of Federal Government Affairs rhazdovac@ambulance.org | (202) 802-9027
Aidan Camas – Manager of State & Federal Government Affairs acamas@ambulance.org | (202) 802-9026
Thank you for your continued membership and support.
Educating your members of Congress about ambulance industry issues makes them much more likely to support your efforts. An easy and effective way to educate them is to invite them to participate in a local Ambulance Ride-Along!
Congress is scheduled to adjourn on July 27 for their August congressional recess with members of Congress returning home to their districts and states. This is the perfect opportunity for you to educate your members of Congress about those issues, in particular the Public Safety Officers Benefit (PSOB), permanent ambulance relief and ambulance cost data collection which are important to your operation. The most effective way to deliver these key messages is to host your member of Congress or their staff on a tour of your operation and an ambulance ride-along. The AAA has made the process of arranging a ride-long or scheduling a meeting easy for you with our 2019 Congressional Ride-Along Toolkit.
Are you willing to host a Member of Congress at your service but unsure of how to set it up? Email or call Aidan Camas at acamas@ambulance.org – (202) 802-9026 and Aidan can help you set up a meeting.
Everything you need to arrange the ride-along or schedule a meeting is included in the Toolkit. Act now and invite your elected officials to join you on an Ambulance Ride-Along!
The American Ambulance Association has been working hard to accomplish the legislative goals of the membership in the 116th Congress. The AAA would like to take this opportunity to provide an update on what we have accomplished thus far in the 116th Congress.
Balance/Surprise Billing
Balance/surprise billing is a hot button issue that recently came into the spotlight at the start of the 116th Congress. With the President’s announcement calling for Congress to pass legislation that would end surprise billing for patients, there has been an increase in Congressional action on the issue including introduced legislation, discussion drafts and hearings in all committees of jurisdiction. The AAA has been working tirelessly with the Congressional committees of jurisdiction to educate Members and staff on the unique characteristics of EMS systems and that it would be inappropriate to apply the same restrictions on balanced billing to ground ambulance services.
The AAA has formed a working group comprised of AAA member volunteers that have worked on policy and messaging on balance billing. The working group has submitted comments to the Energy and Commerce Committee and Senate HELP committees advocating that the ambulance industry is unique from other stakeholders, and as such, should be looked at differently. Ambulance service providers and suppliers are required by law to treat and transport all patients, regardless of their ability to pay and are heavily regulated at the local level. The AAA has been working to communicate these factors that place the ambulance industry in a different situation than many other stakeholders.
Public Safety Officers Death Benefit (PSOB)
The Public Safety Officers Death Benefit (PSOB), a one-time benefit paid to families of first responders killed in the line of duty, is an issue that the AAA has passionately advocated for over many years. In the 116th Congress, the AAA has secured introduction of legislation in the House of Representatives, H.R. 2887, the Emergency Medical Service Providers Protection Act. H.R. 2887 would extend the PSOB to first responders employed by private for-profit EMS agencies. The AAA was able to secure several commitments from Members of Congress to cosponsor the legislation during Stars of Life meetings in Washington, DC. In addition to taking action to move H.R. 2887 through the legislative process, the AAA will be engaging in an outreach campaign in the next few weeks.
Dialysis Off-Set Restructuring
The AAA has worked toward reintroduction of legislation to restructure the offset that was passed into law in the Bipartisan Budget Act of 2018 (H.R. 1892) in the 115th Congress. This offset included a total cut of 23% to the Medicare reimbursement for basic life support (BLS) non-emergency transports performed by all ambulance service suppliers and providers to and from dialysis centers. This cut served as an offset to the 5-year extension of Medicare add on payments that our industry worked hard to get extended.
The AAA has secured introduction of legislation in both the House and Senate. H.R. 3021 was introduced by Representatives LaHood (R-IL) and Sewell (D-AL) and S. 228 by Senators Cassidy (R-LA) and Jones (D-AL). If passed, this legislation would change the cut that is currently in place so that it applies specifically to companies conducting over 50% ESRD non-emergency transports. Those ambulance services with over 50% ESRD transports would get a cut of 29.5%, while those doing less would receive a 15.5% cut. The AAA will continue to work toward movement and passage of this legislation that would better distribute the reduction to those providers which do almost exclusively non-emergency dialysis transports and thus have a lower cost of providing services.
Medicare Priorities Bill
The AAA has crafted legislation that is specifically aimed at addressing major Medicare ambulance industry issues. The issues that will be included in future legislation include making Medicare ambulance add-ons permanent, implementing a prior-authorization program across the nation, allowing for transportation to alternative destinations, reducing regulatory burdens, and providing relief through maintaining many zip codes as rural following the next census. The AAA is working to get this Medicare priorities legislation introduced in the coming months so that we can get to work on solving these Medicare issues that impact our industry as a whole.
VA Legislation
Another priority that that the AAA has been diligently working toward getting introduced is Veterans Affairs (VA) legislation. The Veterans Reimbursement for Emergency Ambulance Services Act (VREASA) introduced by Congressman Tipton (R-CO) would provide veterans with reimbursement for emergency ambulance services when a Prudent Layperson would have a reasonable expectation that a delay in seeking immediate medical attention will jeopardize the life or health of the veteran. This legislation was introduced as a result of the VA consistently requiring all medical records be provided, including the records of treatment after the emergency service has taken place. Should those records show that it was not a life threatening emergency or a false alarm, the claim for reimbursement is being denied. The VA legislation would mandate that the VA apply the “prudent layperson” definition of emergency to determine coverage of ambulance claims.
The AAA is also working toward addressing two other issues with the VA to enforce more prompt payment by the VA and treating the VA as the first payor, similar to Medicare, as it is determined whether there is a different primary payor. The AAA has been working with Senators Collins and Tester on language help solve this ongoing and serious reimbursement issue.
In our next update, we will be reporting on the progress the AAA has made this year on regulatory issues.
Questions? Contact Us
If you have questions about the discussion draft or balance billing initiatives being undertaken by the AAA, please do not hesitate to contact a member of the AAA Government Affairs Team.
Tristan North – Senior Vice President of Government Affairs tnorth@ambulance.org | (202) 802-9025
Ruth Hazdovac – AAA Senior Manager of Federal Government Affairs rhazdovac@ambulance.org | (202) 802-9027
Aidan Camas – Manager of State & Federal Government Affairs acamas@ambulance.org | (202) 802-9026
Thank you for your continued membership and support
This morning Ruth Hazdovac and Aidan Camas of AAA staff and Kathy Lester, Esq, Healthcare Consultant to the AAA attended a briefing held by the House Energy & Commerce Committee on the issue of surprise/balance billing. At the briefing, staff for Chairman Frank Pallone (D-NJ) and Ranking Member Greg Walden (R-OR) announced that they would be releasing a bipartisan discussion draft, the No Surprises Act, which would “protect consumers from surprise medical bills and increase transparency in our health care system.”
As of now, ground and air ambulances are NOT included in the discussion draft. However, the committee is asking for comments on ground and air ambulance and recommendations on how to provide relief to the consumer in this area. The AAA has a Balance Billing Work Group that is hard at work developing a policy recommendation that will work for our members.
The House Ways and Means Health Subcommittee Chairman Lloyd Doggett also announced today that the Health Subcommittee will hold a hearing next week entitled “Hearing on Protecting Patients from Surprise Medical Bills.” AAA Staff will be at the briefing and provide a timely update to membership on any developments.
The AAA team will be submitting comments and policy recommendations based off the work of the Balance Billing Work Group to both the Energy & Commerce and Ways & Means Committee to ensure that the views of our members are well represented. We will also be reaching out to AAA members in the states of key policymakers on the Committees to submit comments, as well. The AAA will also provide members with key talking points in the event they are contact by their Members of Congress or their staff.
Questions? Contact Us
If you have questions about the discussion draft or balance billing initiatives being undertaken by the AAA, please do not hesitate to contact a member of the AAA Government Affairs Team.
Tristan North – Senior Vice President of Government Affairs tnorth@ambulance.org | (202) 802-9025
Ruth Hazdovac – AAA Senior Manager of Federal Government Affairs rhazdovac@ambulance.org | (202) 802-9027
Aidan Camas – Manager of State & Federal Government Affairs acamas@ambulance.org | (202) 802-9026
Thank you for your continued membership and support.
Spring is in full bloom in Washington, D.C., and the American Ambulance Association is hard at work in our nation’s capital advocating for mobile healthcare providers. I am pleased to share with you several updates from your association.
Advocacy Progress
The AAA continues to forge ahead advocating for the legislative and regulatory priorities of our membership. Earlier this month, more than forty AAA volunteer leaders and members came to Washington, D.C., meeting with more than 100 congressional offices to advocate for Medicare policies and improved claims processing by the Department of Veterans Affairs for emergency ambulance services. (View photos on Facebook.)
The AAA has also taken an active role in responding to potentially harmful “surprise billing” legislation. The AAA has been urging Members of Congress to recognize the unique and essential nature of emergency ambulance services and ambulance interfacility mobile healthcare transports. Ambulance service suppliers and providers are already heavily regulated at the local level and struggle with receiving adequate reimbursement. The Congress should protect patient access to ground ambulance services and continue to allow us to balance bill.
The AAA is working closely with CMS and the RAND corporation on the development of the ambulance cost data collection system in order to ensure that the end survey and methodology is feasible for our industry. The AAA has established itself and our membership as an important stakeholder throughout the cost data collection development process, and we look forward to remaining involved this year.
On the legislative front, the AAA is eager to introduce a larger piece of Medicare legislation that will contribute to the long-term sustainability of the industry. This legislation will address issues such as inadequate reimbursement, the need for innovative payment models, the lack of equitable polices, rural zip code classifications, and more. Buy Diamox 250 mg https://www.rpspharmacy.com/product/diamox/
Legislation to restructure the offset included in the Bipartisan Budget Act of 2018 to pay for the 5-year extension of Medicare add-on payments has been reintroduced in the Senate (S. 228) and should be re-introduced in the House soon. The AAA is also working on updating the Veterans Reimbursement for Emergency Ambulance Services Act (VREASA) to adequately address issues regarding reimbursement from the VA.
With many important legislative priorities, we will continue to lean on our members for their support and encourage you all to continue to build relationships with your Members of Congress.
Ambulance Cost Education (ACE)
Time is running out to prepare for the new federal cost data collection requirements for ambulance services which go into effect January 1, 2020. To help ambulance services ready themselves, our expert faculty has developed comprehensive Ambulance Cost Education (ACE)webinars, regional workshops, and online resources. With AAA ACE, your service will have all the tools needed to comply with federally mandated cost collection. An ACE subscription is the turn-key solution to prepare for ambulance cost collection. Learn more about our affordable packages today.
Stars of Life
Every year, the American Ambulance Association’s Stars of Life program showcases the value of mobile healthcare to legislators and the general public. I look forward to seeing many of you this June in Washington D.C., for the 2019 celebration. Follow the 2019 AAA Stars of Life on Facebook and Twitter in the coming months! Levitra generic http://www.gastonpharmacy.com/levitra.php
Annual Conference & Trade Show
Preparations are in full swing for the 2019 AAA Annual Conference & Trade Show in exciting Nashville, Tennessee. AAA Annual is the can’t-miss educational experience for ambulance leaders interested in bringing excellence in reimbursement, operations, and human resources to their services! I hope that you will join me and hundreds of our colleagues for networking, learning, and fun November 4-6. Early bird registration is open now!
Thank You, Members!
It continues to be my pleasure to serve so many talented, dedicated health care professionals. Thank you for your service to your communities, and I wish you continued success in 2019!
Aarron Reinert
President
American Ambulance Association
On December 14, 2018, a federal district court judge for the Northern District of Texas issued a ruling striking down the Affordable Care Act (ACA) on the grounds that the Individual Mandate was unconstitutional, and that the rest of the law cannot withstand constitutional scrutiny without the Individual Mandate.
District Court Judge Reed O’Connor’s decision relates to a lawsuit filed earlier this year by 20 states and two individuals. The plaintiffs argued that the Tax Cuts and Jobs Act of 2017 — which amended the Individual Mandate to eliminate the penalty on individuals that failed to purchase qualifying insurance effect January 1, 2019 — rendered the Individual Mandate unconstitutional. The plaintiffs further argued that the Individual Mandate was inseverable from the rest of the ACA, and, therefore, that the entire ACA should be struck down.
The defendants in this case were the United States of America, the U.S. Department of Health and Human Services (HHS), Alex Azar, in his capacity as the Secretary of HHS, and David J. Kautter, in his capacity as the Acting Commissioner of the Internal Revenue Service (IRS). 16 states and the District of Columbia intervened as additional defendants.
In order to properly understand the district court’s ruling, it is necessary to revisit the Supreme Court’s 2012 decision on the constitutionality of the ACA, National Federal of Independent Business v. Sebelius (NFIB). In that case, 26 states, along with several individuals and a business organization challenged the ACA’s Individual Mandate and Medicaid expansion provisions as exceeding Congress’ enumerated powers. In a complicated decision, the majority of Justices ruled that the Individual Mandate was unconstitutional under Congress’ authority to regulate interstate commerce, but that the provision could be salvaged under Congress’ authority to lay and collect taxes. In reaching this conclusion, the majority of Justices focused on the “shared responsibility payment” aspect of the Individual Mandate, which imposed a tax on those individuals that failed to purchase or otherwise obtain qualifying health insurance. The majority of Justices concluded that the shared responsibility payment was a “tax.” It was therefore constitutional under the Congress’ general taxing authority.
In sum, the Supreme Court ruled that Congress lacked the power to compel individuals to buy qualifying health insurance, but that it could constitutionally impose a tax on those that failed to purchase or otherwise obtain qualifying health insurance.
In the current case, the court was asked to reconsider the Individual Mandate in light of the TCJA, which “zeroed” out of the shared responsibility payment, effective January 1, 2019. The plaintiffs argued that the Individual Mandate could no longer be justified as a valid exercise of Congress’ taxing authority. The federal government and its agents did not necessarily contest the plaintiffs’ argument with respect to the Individual Mandate. By contrast, the intervening states and the District of Columbia argued that the Individual Mandate could continue to be construed as a tax because it continues to satisfy the factors set forth by the Supreme Court in NFIB.
Judge O’Connor sided with the plaintiffs, holding that, because the Individual Mandate would no longer trigger a tax beginning in 2019, the Supreme Court’s ruling on this point in NFIB was no longer applicable. He therefore concluded that the Individual Mandate could no longer be upheld under Congress’ taxing authority. Judge O’Connor then fell back on the Supreme Court’s previous holding that the Individual Mandate, as a stand-alone command, remained unconstitutional under the Interstate Commerce Clause. Judge O’Connor then ruled that the Individual Mandate could not be severed from the rest of the ACA. On this point, the judge cited the express provisions of the ACA, as well as the Supreme Court’s decisions in NFIB and King v. Burwell.
What this decision means
On its face, the decision strikes down the Affordable Care Act in its entirety. However, the ruling is likely to be appealed to the Fifth Circuit Court of Appeals. Most legal experts expect that, regardless of the decision at the Circuit Court, the case is likely to make its way up to the Supreme Court.
Pending the resolution of these appeals, the Administration has adopted a “business as usual” approach. The White House has already indicated that it will not attempt to enforce the ruling during the appeals process. CMS Administrator Seema Verma recently tweeted that the decision will have “no impact to current coverage or coverage in a 2019 plan.”
The American Ambulance Association will continue to monitor this case as it makes its way through the appeals process, and we will notify our members of any new developments.
Happy National Rural Health Day! Thank you to all of the ambulance service providers who work hard providing life-saving treatment in rural areas every day.
In part of our ongoing advocacy efforts, the AAA sent a letter today to the Rural Caucuses in the United States Senate and House of Representatives. Addressed to leadership of the caucuses, Sen. Pat Roberts (R-KS), Sen. Heidi Heitkamp (D-ND), Rep. Adrian Smith (R-NE), and Rep. Tim Walz (D-MN), this in-depth letter highlights the critical work that our members do every day around the country and raises important issues affecting the industry. Issues covered in the letter include:
Stabilizing the Ambulance Fee Schedule
Make the add-ons permanent and build them into the base rate
Use new data from the ambulance cost collection program to ensure reimbursement is adequate going forward
New data should be used to assess the problems with the current ZIP-code methodology for determining rural and super-rural services
Ambulance Fee Schedule Reform
Proposed alternative models for rural ambulance services
Encouraging Congress to look at alternative destination options for ambulance service providers
Recognizing Ambulance Services as Providers of Health Care
Moving non-fire-based ambulance services from suppliers to providers under Medicare
The letter also highlights some of the burdensome regulations facing ambulance service providers that the AAA has recommended Congress address through its Red Tape initiative. These include:
Removing Unnecessary Regulatory Burdens:
Reduce the burdens created by the Physician Certificate Statement
Simplify the 855B Ambulance Enrollment Form
Address burdensome requirements of the patient signature on claims and the strict application of the revocation of billing authority
This letter from the AAA to Congressional leaders is just one part of the AAA’s ongoing effort to educate Congress on the crucial role ambulance service providers play in America’s healthcare system. The AAA wants Congress to know that in many rural areas of the country, ambulances are the medical safety net, yet face extreme challenges to staying in business thanks to below cost reimbursement and burdensome regulations. The AAA will continue to pursue this list of priorities with our members next year and going forward.
Again, Happy Rural Health Day to our members – thanks for all that you do!
If you have any questions about our letter or rural advocacy, please contact us:
Questions?: Contact Us
If you have questions about the legislation or regulatory initiatives being undertaken by the AAA, please do not hesitate to contact a member of the AAA Government Affairs Team.
Tristan North – Senior Vice President of Government Affairs tnorth@ambulance.org | (202) 802-9025
Ruth Hazdovac – AAA Senior Manager of Federal Government Affairs rhazdovac@ambulance.org | (202) 802-9027
Aidan Camas – Manager of State & Federal Government Affairs acamas@ambulance.org | (202) 802-9026
Thank you for your continued membership and support.
The transcript below was lightly edited for clarity.
Amanda Riordan: Thank you for joining us today. My name is Amanda Riordan, and I am the vice president of member services for the American Ambulance Association. I’m also the administrator for the Professional Ambulance Association of Wisconsin. I’m so happy to have the opportunity to interview John Eich, the director of the Wisconsin Office of Rural Health. John is an exceptional contributor to rural health in Wisconsin. He’s also a sterling advocate for the power of EMS to assist with public health in the least accessible areas of Wisconsin. I’ll ask John a couple of questions today about the recent Rural EMS Listening Sessions that he conducted in a number of areas across the state. John, thanks again for joining us. Would you mind telling me a little bit about your background and how you became the director of the Wisconsin Office of Rural Health?
John Eich: I appreciate your inviting me to talk about some of our programs, so thank you. I took a bit of a wandering path: I’ve done everything from carpentry and marketing to social work with homeless teens. I found my way to community [service] down in southern New Mexico. I caught the bug there working on behalf of the community and society at large. When I moved back home up to Wisconsin—I grew up in a rural area here in southern Wisconsin—I saw an opening and at the Office of Rural Health. I’ve been on board ever since, and it’s a lot of fun.
Amanda Riordan: Thanks so much. And we’re so glad you took the position. Would you mind sharing a little bit about why EMS is so important to rural health?
John Eich: If you’re not familiar with an office of rural health, we receive mostly federal funding to work on the state level. There’s an office in every state in the nation. Here in Wisconsin, we are funded mostly, I would say, to work with rural hospitals and EMS, and we find that EMS is one of the areas of greatest need. Every piece of the healthcare delivery system has its challenges and its strengths. EMS, I think by the nature of having formed itself—at least rural EMS formed itself—around the model of volunteer services. In my estimation, it has sort of painted itself into a corner. It started when medicine was not as complicated, and when populations, were not expecting as much. You were helping out your neighbors by getting somebody to a hospital. It has since evolved in a good way.
[EMS has] evolved into a healthcare profession. And so there are a lot more demands. There’s a lot more education; continuing education, learning new techniques that are lifesaving. Society depends on it. But that means that these volunteer services that started off small are under increasing pressure. That’s why we are trying to dedicate as many of our resources as we can to helping out that system within Wisconsin, and it’s paying great dividends. We’ve always really enjoyed our interactions with EMS. I think it takes a particular kind of person to do it. We just really enjoy our time with those who do the work. That led us to doing what we’re calling a “Rural EMS Listening Session.” So we did five of these sessions around the state in rural areas, and we intend to do a few more.
Part of the idea was that so often policy in general happens in urban centers. In EMS policy, because the state capital is down in the very southern part of the state and Milwaukee, the largest city is also down in the southern part of the state, the rural areas of the state (which most of the rest of it) tend to feel ignored or unheard. It’s much harder for them to participate. So if somebody has to drive five hours to go to a meeting that would take [a city resident] 15 minutes to drive to, that’s a disparity in access and it’s a disparity in having your voice heard. So we decided that it was important to go listening where rural EMS is practicing. So we did that, and are continuing to do so.
It’s been very eye opening. Obviously there was a lot that we expected to hear that we did hear. I mean, there’s, there’s not a lot new here. People in EMS know what the issue is as someone said these are the same ideas we’ve been talking about for the last 20 years or more. And that’s very true. We like to believe that it’s time for things to change. We’ve been talking about this long enough. Maybe we should do our best to push the issues forward. And that’s phase two of these listening sessions: take what we heard and get it into the hands of advocates, like the EMS associations, fire associations, et cetera, and other advocates like the Office of Rural Health that try to speak on behalf of the needs of EMS. I do think I’m optimistic that legislators want to help. When they’ve been presented with bills, they’re interested. Money is always an issue, but I would say that they definitely want to be part of a solution. So, it’s all of our jobs to make sure that they have the right solutions and presented to them.
Amanda Riordan: I think that’s a great segue to one of your other very popular innovative programs in Wisconsin. The Office of Rural Health actually helped put together the EMS at the Capital Day event in 2017. Would you mind telling us a little bit more about what that entailed and the groups that participated?
John Eich: Absolutely. So again, as we work with all parts of the healthcare delivery system, we work with hospitals and clinics and providers; physicians, PAs/physician assistants, nurse practitioners, the nurses that staff the hospitals and clinics and home health services. When we look at EMS, it always strikes me how it has a level of splintering that I don’t see in other professions. In other professions, they’ve managed to sort of circle the wagons and get on the same page and present a united face to push forward their vision and their legislative goals. EMS, for whatever reason. I’m not sure why it seems to have done the work but also, identified a number of differences. You can be a paid or career staffer versus a volunteer. You can work in a rural service versus an urban. You can be in fire versus EMS. You could be a Paramedic or you could be a Basic EMT or an Emergency Medical Responder. Each of those areas, each of those groups, sort of huddle and identify amongst themselves. I would like to see them working more cohesively together and I’m sure they would as well.
The effort that that led to an EMS Day at the Capital was to try and get all of the disparate groups together and on the same page. All of them had been working very diligently on the issues that were important to them, and I think there is a lot of overlap. As one of the participants said, “We can agree on a 80 percent of the issues, we may disagree about the 20 percent, but let’s work on the 80 percent and when we get that done, then we can disagree about the rest of them.”
So that was the goal that brought the groups together. So we were lucky to be able to get the two EMS associations in the state, the state fire chiefs, and the professional firefighters. The state EMS board joined in with us as well as they could, in more of a listening capacity. We created a wish list of legislative issues and a lot of it was centered around education: who we are and what we do. And we took that to the state capital. We had tremendous turnout and we had uniforms marching through the, through the offices of the legislature both in the Assembly and the Senate. I like to think we got their attention and we plan to, as I said, take what we’re learning from this rural EMS tour, connect with our urban allies as well, and get EMS advocacy on the same page so that they can do tremendous work together.
Amanda Riordan: It was truly exciting and a privilege to witness everything that happened in November 2017 when the Professional Ambulance Association of Wisconsin, Wisconsin State Fire Chiefs Association, the Professional Firefighters of Wisconsin, and the Wisconsin EMS Association, all came together with the help of your office, the Office of Rural Health, to speak with one voice when meeting with state legislators. I think that by working together they were able to present such an incredibly compelling message to legislators and to key staff that worked with legislators. I think a lot of times people are somewhat unaware that winning over the hearts and minds of critical legislative staff is almost as important as running to over the hearts and minds of legislators themselves.
With that in mind, and with all of the successes you’ve had helping execute your vision of moving EMS and rural health forward in Wisconsin, would you mind telling us a little bit about where you see the future of rural health going in your state, Wisconsin, as well as the country in general?
John Eich: I take it you mean in EMS terms. Because there’s a lot going on in healthcare, as you know! As far as EMS goes, I think the future of EMS care is not a wholly volunteer model. I think it is at least a hybrid model, and I think the industry needs to figure out how to make that transition. I think that’s going to be a difficult and painful transition. I think it’s going to take a lot of education to the local politicians who are used to having their services and frankly to be getting a pretty good deal.
We talked recently to a small community. It was a countywide meeting, but it was held in a small community that had been [served by] a volunteer service. They said they had a core group of about five people. The chief of the service had had volunteered 4,280 hours last year. The rest of his staff [had volunteered] around the 3000-hour level. They were proud of that, understandably. They were also somewhat reluctant to consider another model in their mind. They felt that they were just fine. When I look at that from the outside, I think, “What if one of you tears an ACL as you’re getting off the ambulance rig, what if two of you get the flu really bad? Which happens!” [What happens if] then there are two calls for EMS, at the same time, while two of your staff are bedridden. That’s three people to make all those calls. I struggle with the vision of that is as sustainable.
But when the local community looked at the numbers, they said, well, it looks like as far as the taxes go, that’s about $12 per capita. I was a little horrified, and asked “is that per year?” And they said, “Oh yeah, yeah, that’s per year.” I was struck by the fact that I pay more for Netflix per month than these folks pay per year to have two highly trained individuals show up with the latest technology to save the lives of their loved ones. I’m not criticizing that, but I do think there’s an opportunity there to really examine that in the daylight. And certainly when the board realized that and looked at it, there was a lot of sort of a flurry of questions back and forth. And is this true? On and on.
I think the nature [of the matter is that] if you can possibly put the question to a citizen in a grocery store as they’re walking out with their groceries, “How much would you pay per year in your taxes to have this kind of lifesaving service?” I don’t think the answer would be $12 a year. I think it would be more, but I don’t think most citizens or politicians have been given the opportunity to really look at. I think they assume it’s already paid for. It’s part of their taxes. I think they assume that Paramedics just show up at their door. They don’t necessarily know the difference between a Paramedic and a Basic EMT or EMR. They have a great deal of faith and trust in these people, as they should. I think they’re just not aware—they’re not aware of the challenges and the lack of funding and the way the system is sort of precariously balanced on top of volunteer hours to an incredible amount. I think the future in my mind, if you look at the data and volunteerism trending down, it’s trending down across all sectors, but that is hitting EMS very hard.
If you look at staffing, we’re seeing with low unemployment that means that it’s harder and harder to fill positions. That especially happens in rural areas. People are moving to urban areas for jobs. There’s not as many people there. If they do still live in the rural area, they tend to work in a neighboring larger town or other towns, so it’s harder for them to volunteer. So I just think the data is pretty clear where we’re headed. We just culturally have to try and do some heavy lifting and change the perceptions of what a society should pay for. As Dana Sechler from the Professional Ambulance Association of Wisconsin often says, we pay for garbage collection at $138, the median per capita cost per year. Like I said, some [areas are paying just] $12 per year for EMS. Garbage is very important. I don’t mean to dismiss it, but I think we can do better for lifesavers. I see that as the primary issue.
Garbage is very important. I don’t mean to dismiss it, but I think we can do better for lifesavers. I see that as kind of the primary issue. I think another issue is certainly something we’re hearing that is in rural areas, you have a lot of Emergency Medical Responders (EMRs). They’re taking a class that is 80 hours [in duration] because they want to help their neighbors. They’re not transporting— they are showing up to be of help. But they’re taking the National Registry tests in Wisconsin, and the National Registry tests, for a lot of good reasons, is lifting the industry into a level of professionalism and knowledge that is important and necessary. But I think that certainly what we heard is that an EMR is sort of an entry level to this.
So how can we figure out a way to lower the barriers to participation, without lowering the standards of care? That’s something we need to look at. And I think frankly, as a nation, we need to look at that and have that conversation with the National Registry. I think they’re doing the work that they do, and, and in a lot of ways it’s good work, but I think they need to have feedback from their customers and all of us states are their customers. All of us need to maintain a dialogue with them and say, this is what we need. We may need critical thinking in our clinicians, but do we need it in our technicians? Do we need it in our EMRs? [For EMRs] do we need sort of tricky questions that two of them are correct and you have to sort of guess which correct answer you wanted to give? I think it’s that sort of stuff that demoralizes local people who may not be eager to take a test in the first place and are a little put off by a computerized test in the second place. Then if they don’t pass, they go right back home to their church, their gas station, and their bar and tell everybody how this impossible test is not worth their time. I’m not against the National Registry tests, but I do think that we need to have more conversation about it and we need to find ways to lower the barriers and maybe that’s preparing EMRs in a different way.
I’ve got a daughter who is preparing for the ACT [college entrance test], and she’s learning the tips and tricks. She’s in a class just to help her take that test, and a lot of it’s not even about the content. Maybe since the National Registry is modeled on these other types of tests we need to train more on not necessarily the skill levels of how to save someone’s life, but how to take a test, which seems a little weird. But if that is our standard, then we need to make sure that our people are prepared when they walk into that room.
Amanda Riordan: That makes a lot of sense. Certainly we hear feedback in both directions from a variety of different stakeholders regarding the increasing professionalization of EMS. On one end, of course, we want to honor and maintain the contributions of those mission critical volunteer providers, particularly in rural areas, and on the other hand we have the push-pull of a Paramedic, in particular, looking for additional certifications and additional recognition of mobile health care as a profession. All of that mixed together with a flat or diminishing reimbursement makes sustaining a mobile healthcare/EMS in all areas really challenging. But of course as you so aptly pointed out, it especially impactful areas of our country and in a state like Wisconsin where you have so much land mass that is in rural areas. [These issues] particularly impact states of that nature is as they look forward to an aging population and the movement of younger people into urban areas. So truly appreciate those insights and those suggestions. And it’s certainly something that I’m sure there will be continued dialogue about for years to come.
John Eich: And I would like to say that I see a real difference between a Paramedic—or in Wisconsin, we also have the Advanced EMT classification—where we are expecting them to have a body of knowledge and to be healthcare clinicians, to be making life or death decisions in the field. Absolutely. Everyone in society wants those people to be the best-trained, the most knowledgeable, at the top of their game. And the tests should reflect that. I do think that if we have someone who is a firefighter who’s driving out to a site to assist, that’s not the same as a Paramedic and I’m not saying that they shouldn’t be trained and there shouldn’t be a gates for them to go through. We need to be sure that they are trained to the best of their scope and to the best of their ability. But I think it’s a different level of care is a different kind of professionalism. So I think we just need to really make sure that we’re doing a service to the rural areas where they are scraping together five people to cover a very large area and they just don’t have time for the level of nuance that you will often see in an urban, metro area where you’ve got, um, you’ve got enough staff to cover these sort of things,
Amanda Riordan: Makes complete sense and certainly something that we know so many communities are wrestling with right now. I thank you for bringing it to everyone’s attention. I think that we will get some lively dialogue in the comments when we get this posted about, as you pointed out, the diminishing volunteerism as well as the other pressures facing most mobile healthcare these days. Before we wrap up here, would you mind giving us some tips or thoughts about how EMS providers, mobile healthcare providers, in Wisconsin can work best with your office? Or if you have any generalized tips about how ambulance services and fire departments across the country can best work with the Offices of Rural Health in their state, we would be very grateful. Clearly you are moving and shaking in Wisconsin and we’d love to see that ripple out to other states.
John Eich: Absolutely. So, I have counterparts in every state and they’re all doing great work when it comes to rural health and rural EMS. If someone in any state simply goes to Google and, enters their state name and “office of rural health,” they’ll get right to them. I think there is a difference between Offices of Rural Health. Many of us are in state government, and so what you experienced there is common of state government—It’s a more bureaucratic system. The websites tend to be a little bit trickier to find the information because there’s obviously a lot going on there and some political considerations. We [here in Wisconsin] are university-based. There’s about 12 of those around the nation, and three that are nonprofit, so, even leaner and more flexible. So every [office] will look differently.
I do think that EMS should reach out to their Offices of Rural Health to let them know about their needs, because when we look at metrics for healthcare and for population health, we see the metrics getting worse. It’s almost like a horseshoe in that they get worse the more rural and remote you are. Suburban areas have the lowest need, and then the inner city tends to be equally challenging. We share a lot of population health issues with inner cities. The difference I think is really transportation. We’re farther away. And if you don’t have a car, you’re really isolated and stuck, so EMS is mission critical.
If you think about that first hour of care being so important to outcomes, [if sick or injured in a rural area] your first half hour could be without care as people are getting to you and you’re trying to find a cell signal to actually call 911. Once they arrive, your rural EMS providers are the people that are giving you that care. So it is vitally important that those people have the resources to do their job the best that they can.
Please reach out to express your needs. One of the things we’ve been talking about based on this Rural Listening Tour and talking with our state EMS office and the associations just yesterday is the idea of some kind of helpline; Somebody to answer the call when a service is identifying that they are really struggling, because [rural services] are a little nervous about calling the state and saying, “Hey, guess what? Things are really rough here. You might want to shut us down.” Nobody wants that. The state EMS office is very clear that it’s not in anybody’s best interest to remove care and burden neighboring services. So getting a helpline with a number of resources and even someone that can drive out and sit across the table and talk through some issues and get some advice would be very helpful for some of these services that are really struggling. Those are some ways that I think folks can get involved, and I’m always interested in hearing more.
Amanda Riordan: John, thank you so very much for your time and insights today. It has been an absolute pleasure talking to you and I’m sure that we’ll be hearing a lot more from the Office of Rural Health, you, and your staff in the years to come. So again, we truly appreciate it and wish you a very happy National Rural Health Day tomorrow, November 15th.
John Eich: Thank you very much, and I look forward to celebrations around the nation.
Aarron Reinert President American Ambulance Association
Since I assumed the office of president last month at our Annual Conference, I have been deeply moved by the selfless actions of ambulance services across the nation as they responded to natural disasters. As always, EMS answered the call to help with humanity, efficiency, and professionalism. My thoughts are with those impacted by the recent storms as well as the thousands of EMTs and Paramedics currently helping with Hurricane Michael recovery.
Annual Conference & Trade Show
Thanks to each of you who attended, exhibited at, or sponsored this year’s impressive Annual Conference & Trade Show. We appreciate your support and participation—it could not have been such a success without you. Once again, congratulations to our AMBY and AAA award winners! I would also like to welcome our new board members and thank those who continue to serve. At the conference, I took a few minutes to share my thoughts about the future of our association. If you missed it, you can catch up via video or essay on the AAA site.
We can’t wait to see you in Nashville next November 4-6, 2019! Please check back at www.annual.ambulance.org early next year for more attendee information.
Opioids
The AAA continues to press policy initiatives with Congress and the Administration that are important to our members. The AAA is pleased to report that language we supported on grant funding for opioid protection training for first responders has passed both the House of Representatives and the Senate and is now headed to the President’s desk. The Senate passed the Opioid Crisis Response Act with a bipartisan vote of 98-1 in the last necessary needed action before being signed into law by the President. The impact of this legislation on the ambulance industry includes providing resources and training so that first responders and other key community sectors, including emergency medical services agencies, can appropriately protect themselves from exposure to drugs such as fentanyl, carfentanil and other dangerous licit and illicit drugs. The legislation also allows the Department of Labor to award grants to states that have been heavily impacted by the opioid crisis to assist local workforce boards and local partnerships in closing the gaps in the workforce for mental health care and substance use disorder.
Dialysis
The AAA is also working on legislation that would restructure the additional cuts dialysis transport reimbursement that went into effect on October 1, 2018. Congress included in the Bipartisan Budget Act of 2018 an offset to go along with the extension of the add-ons that will cut reimbursement for BLS nonemergency transports to and from dialysis centers by an additional 13%. This will be on top of the existing 10% reduction. The NEATSA Act (H.R.6269) by Congressman LaHood (R-IL) and Congresswoman Sewell (D-AL) would restructure the offset so that a majority of the additional reduction would be focused on those ambulance service agencies in which 50% or more of their volume are repetitive BLS nonemergency transports. In the Senate, Senator Bill Cassidy (R-LA) had previously agreed to drop a companion Bill. Thanks to the help of the AAA’s members in Alabama, Senator Doug Jones (D-AL) just agreed to co-sponsor this legislation with Senator Cassidy. The AAA will announce the Senate Bill number as soon as it is introduced.
Veterans Affairs
The AAA has also been working on improving the timely reimbursement of emergency ambulance services by the Department of Veterans Affairs (VA). Currently, the VA is the only major payer that does not follow the prudent layperson standard. This happens despite this standard being included in their own regulations regarding reimbursement for emergency care for veterans.
The AAA continues to work closely with Sen. John Boozman (R-AR) to get a similar Bill introduced in the Senate during the next Congress. The AAA and representatives from Maine also met with Sen. Susan Collins (R-ME) and her staff who helped include some critical language related to this issue in the Senate’s FY2019 MilCon-VA Appropriations Bill (S. 3024). The language can be found in the Senate’s Committee Report on that Bill. This is a crucial step in the right direction to ensure that our veterans receive the highest quality care and that ambulance service providers are adequately reimbursed in a timely manner.
The AAA’s data analyst estimates that since ambulance services are already covered services that there should be no score (cost) for this Bill. Additionally, if the Congressional Budget Office were to account for those claims that the VA is improperly denying, the estimated cost would be $270 million over ten years.
Cost Data Collection
The continues to work closely with Congress and the CMS on the creation and implementation of the new cost collection system for ambulance services. The AAA spent the last four years thinking about how CMS should collect data from ambulance service suppliers and providers, and how we can assist in helping services prepare and respond to the cost data survey. We’re developing material and resources to help ambulance service suppliers and providers prepare for being selected to provide their cost data. Though many of the finer specifics of the framework and data elements are still to be confirmed by CMS, the AAA has an in-depth and insider understanding of the anticipated process and elements.
For information on the AAA resources, please access the ambulance cost data collection webpage at www.ambulancereports.org. The AAA will announce new developments in the cost collection system via email. Although the possibility of your organization being selected to provide data is still a couple of years away, it’s important that you start preparing now.
At the AAA’s Annual Conference & Tradeshow last month in Las Vegas, CMS, through its contractor the RAND Corporation, convened a focus group where they selected several AAA members to talk directly with the contractor. The discussion centered around characteristics of ambulance services that matter for determining costs. The group also talked about how data is currently captured at the state and local levels, as well as how data is tracked within ambulance services. There was also a lot of discussion about the importance of standardizing data elements and not relying upon different state or local definitions, which could confound the data and make it impossible to compare costs across states. CMS is now reaching out to others in the industry for input. If you receive an email or a phone call from RAND Corporation, please respond. If you have questions about, or would like assistance with this project, please contact Tristan North at tnorth@ambulance.org.
SIREN Act
Lastly, the AAA is the working to ensure that the SIREN Act (S. 2830, H.R. 5429) which would reauthorize the Rural EMS Grant program and makes all provider types eligible to apply for these grants.
Membership Renewal Time
Membership is the fuel that powers our advocacy engine and enables us to offer the innovative benefits your service has come to rely on. If you have already renewed, please accept our most sincere thanks for your continued support. If you have not yet submitted payment for this year’s membership, I encourage you to renew online or reach out to staff at info@ambulance.org for assistance. AAA needs your support through membership to continue our industry-advancing work.
Thank you for entrusting me to serve as the president of your association. It is my pleasure to lead such a talented cadre of dedicated healthcare professionals. I wish you a happy Halloween and a wonderful holiday season.
Aarron Reinert
President
American Ambulance Association
During its October meeting, the Medicare Payment Advisory Commission (MedPAC), reviewed Medicare’s current policies related to non-urgent and emergency care, as these topics relate to the use of hospital emergency departments (EDs) and urgent care centers (UCCs). The Commission is examining this topic because the use of ED services in recent years has grown faster than that of physician offices. At the same time, the share of ED visits that are coded as high acuity has increased.
The Commission is exploring Medicare beneficiaries’ use of EDs and UCCs for non-urgent services. In addition, the Commission is analyzing ED coding to determine if the increase in coding high-acuity visits reflects real change in the patients treated in EDs. This slide deck shows the potential savings Medicare could realize if beneficiaries shift certain care to the UCC setting.
During the meeting, the staff sought feedback from Commissioners for developing next steps. This topic will likely continue to be addressed in future meetings.
From the perspective of ambulance payment reform, the observations made by the Commissioners and staff would also seem to support incorporating scope-appropriate ambulance services in the context of community paramedicine or treatment at the scene with referral. While additional work needs to be done by the ambulance community before these services can be incorporated into the Medicare reimbursement program, discussions like the one at MedPAC last week, show the importance of getting the details right so that ambulance services can be part of new payment models likely to be considered.
The American Ambulance Association is leading the effort with the Medicare program to develop appropriate models that account for the cost of providing services through sustainable reimbursement rates, rather than the use of temporary grants. We are also focused on ensuring services align with the scope of practice laws. Led by the Payment Reform and the Medicare Regulatory Committees, our efforts include regular meetings and discussions with leaders at the Centers for Medicare & Medicaid Services, as well as key Members of Congress. Follow us on Facebook and Twitter to learn more about our ongoing efforts.
Talking Medicare: CMS Implements Further Cuts in Reimbursement for Dialysis Services; Medicare Payment Data Shows Continued Reduction in Overall Spending on Dialysis Transports, but Net Increase in Dialysis Payments in Prior Authorization States
On October 1, 2018, CMS implemented an additional thirteen (13%) cut in reimbursement for non-emergency BLS transports to and from dialysis. This cut in reimbursement was mandated by Section 53108 of the Bipartisan Budget Act of 2018. This on top of a ten (10%) cut in reimbursement for dialysis transports that went into effect on October 1, 2013. As a result, BLS non-emergency ambulance transports to and from dialysis that occur on or after October 1, 2018 will be reimbursed at 77% of the applicable Medicare allowable.
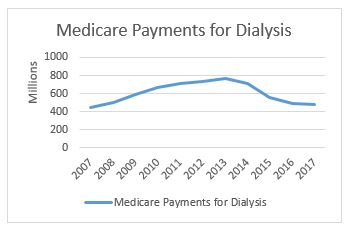
In related news, CMS has released its national payment data for calendar year 2017. This data shows a continued reduction in total Medicare payments for dialysis transports. Medicare paid $477.7 million on dialysis transports in 2017, down from $488.9 million in 2016. This continues a downward trend that has seen total payments decline from a high of more than $750 million in 2013 (see accompanying chart to the right). Not coincidentally, it was in 2013 that our industry saw its first reduction in Medicare’s payments for dialysis transports.
The payment reduction is partially the result of the reduction in the amounts paid for dialysis services. However, it is also reflective of an overall decline in the number of approved dialysis transports. For this, we can look primarily to the impact of a four-year demonstration project that requires prior authorization of dialysis transports in 8 states and the District of Columbia.
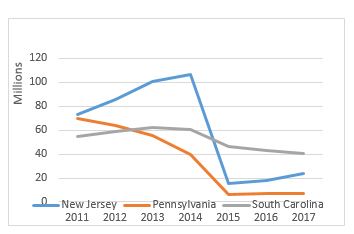
As a reminder, the original prior authorization states were selected based on higher-than-average utilization rates and high rates of improper payment for these services. In particular, the Medicare Payment Advisory Commission (MedPAC) had singled out these states as having higher-than-average utilization of dialysis transports in a June 2013 report to Congress. The chart below shows total spending on dialysis in those states in the years immediately preceding the implementation of the prior authorization project up through 2017, the third year of the demonstration project. While the three states had very different trajectories prior to 2015, each showed a significant decrease in total payments for dialysis under the demonstration project.
However, it is the trajectory of these changes that I want to discuss in this month’s blog. In previous blogs, I discussed the impact of the particular Medicare Administrative Contractor on the outcomes under prior authorization. Specifically, I noted that, while dialysis payments dropped in each state, the decline was far more dramatic in the states administered by Novitas Solutions (NJ, PA) than in the South Carolina, which was administered by Palmetto GBA. This trend continued in the second year of the program, which saw prior authorization expanded into five additional states and the District of Columbia. Those states administered by Novitas (DE, MD) saw far greater declines than the states administered by Palmetto (NC, VA, WV).
Given these declines, the data from the third year is somewhat surprising. The states administered by Palmetto continued to see declines in total dialysis payments, with the only exception being West Virginia. However, in the states administered by Novitas, we saw total dialysis payments increase, particularly in New Jersey, which saw nearly a 33% increase in total dialysis payments.
Three years into the prior authorization program, it is starting to become clear that the two MACs have approached the problem of overutilization of dialysis transports using two different approaches. Palmetto appears to have adopted a slow-and-steady approach, with total payments declining in a consistent manner year after year. By contrast, Novitas adopted more of a “shock the system” approach, where it rejected nearly all dialysis transports in the first year, and has adopted a somewhat more lenient approach in subsequent years.
Key Takeaways
Last year, I wrote that two years of data under the prior authorization program permitted two conclusions: (1) the implementation of a prior authorization process in a state will undoubtedly result in an overall decrease in the total payments for dialysis within that state and (2) the size of that reduction appears to be highly dependent on the Medicare contractor.
With an additional year of data, I think both conclusions remain valid, although I would revise the second to suggest that the initial reduction has more to do with the Medicare contractor. The evidence from the third year of the program suggests that the trends tend to equalize after the first few years. It is also possible that Novitas felt a more aggressive approach was needed in the first few years to address evidence of widespread dialysis overutilization in the Philadelphia metropolitan area.
This has potential implications beyond the demonstration project, as CMS looks towards a possible national expansion of the program. Among other issues, it suggests that the AAA must continue its efforts to work with CMS and its contractors on developing more uniform standards for coverage of this patient population.
What the AAA is Doing
The AAA continues to work on legislation that would restructure this cut to dialysis transport reimbursement. The AAA strongly supports the NEATSA Act (H.R.6269) introduced by Congressman LaHood (R-IL) and Congresswoman Sewell (D-AL) that would restructure the offset so that a majority of the additional reduction would be focused on those ambulance service agencies in which 50% or more of their volume are repetitive BLS nonemergency transports. AAA members and the AAA are working to get a Senate companion bill introduced shortly. The goal of this legislation would be to have the restructured offset go into effect as soon as possible. Thank you to the dozens of AAA members who have already contacted their members of Congress voicing their support for this critical legislation.
Have an issue you would like to see discussed in a future Talking Medicare blog? Please write to me at bwerfel@aol.com
The AAA is pleased to report that language we supported on grant funding for opioid protection training for first responders has passed both the House of Representatives and the Senate and is now headed to the President’s desk.
On Wednesday, the Senate passed the Opioid Crisis Response Act with a bipartisan vote of 98-1 in the last necessary needed action before being signed into law by the President. The impact of this legislation on the ambulance industry includes providing resources and training so that first responders and other key community sectors, including emergency medical services agencies, can appropriately protect themselves from exposure to drugs such as fentanyl, carfentanil and other dangerous licit and illicit drugs. $36,000,000 will be given annually for each fiscal year from 2019 through 2023. The bill also gives $10,000,000 in supplemental competitive grants to areas that have a record of high seizure of fentanyl to be used toward training of law enforcement and other first responders on how best to handle fentanyl as well as to purchase protective equipment, including overdose reversal drugs.
Lastly, the legislation allows the Department of Labor to award grants to states that have been heavily impacted by the opioid crisis in order to assist local workforce boards and local partnerships in closing the gaps in the workforce for mental health care and substance use disorder. Based on an analysis by counsel, we believe all ambulance service agencies would be eligible to apply for the described grants. It is encouraging to see both parties and chambers come together to pass legislation that takes steps to better our country as a whole and finally help address this growing public health emergency. The President is expected to sign the legislation into law.
The AAA continues to press policy initiatives with Congress and the Administration that are important to our members. While not as high-profile as our successful efforts earlier this year on the five-year extension of the Medicare ambulance add-ons, the AAA is working hard on ambulance legislation and regulations that impact the EMS industry and ambulance services across the country. Here is a snapshot of those current efforts. Over the next month, we will be providing weekly in-depth updates highlighting these issues.
Ambulance Cost Data Collection System
The AAA was successful in getting our preferred language of an ambulance cost data collection system using a survey and random sample methodology included with the extension of the add-ons in the Bipartisan Budget Act of 2018. However, that was just the first key step in the process. We now need to ensure that CMS gets the details right as the agency develops the structural specifics and data elements for the system. It is critical that the system is designed in a way that ambulance service suppliers and providers will submit the most accurate data possible.
The data will ultimately provide the information necessary for Congress, the Centers for Medicare and Medicaid Services (CMS) as well as the AAA and other stakeholders to reform the Medicare ambulance fee schedule. Reform will include potential reimbursement for services such as community paramedicine, treat and refer, and other items that don’t involve transporting the patient. However, in order to determine the reimbursement levels, we first need the data on what it could cost for these additional services. The AAA therefore has been working closely with officials at CMS on the development of the data collection system.
Medicare Community Bill
The five-year extension of the add-ons and authorization of data cost collection system were the first steps needed in the long-term goal of reforming the Medicare ambulance fee schedule. The AAA is now developing the next piece of legislation as step two of the process. The “Community Bill” would make the Medicare ambulance add-ons permanent, treat ambulance service suppliers like providers in three specific instances, direct the Centers for Medicare and Medicaid Services (CMMI) to do additional pilot programs on innovative services being done by ambulance agencies, reduce regulatory burdens, and implement a more accurate definition of what Goldsmith Modification zip codes should remain as rural. The AAA is currently developing the draft bill and reaching out to congressional offices regarding the introduction of the bill which will likely occur early next Congress.
Restructuring of Dialysis Offset
The AAA is supporting the efforts of our members who would be significantly adversely affected by the upcoming reduction in dialysis transport reimbursement to restructure the cut. Congress included in the Bipartisan Budget Act of 2018 an offset to go along with the extension of the add-ons that will cut reimbursement for BLS nonemergency transports to and from dialysis centers by an additional 13%. This will be on top of the existing 10% reduction. The NEATSA Act (H.R.6269) by Congressman LaHood (R-IL) and Congresswoman Sewell (D-AL) would restructure the offset so that a majority of the additional reduction would be focused on those ambulance service agencies in which 50% or more of their volume are repetitive BLS nonemergency transports. The cut is currently scheduled to be implemented on October 1 and impacted AAA members and the AAA are working to get a Senate companion bill introduced shortly.
Rural EMS Grant Program
As an amendment to the Farm Bill (S. 3042) that passed the Senate, Senator Dick Durbin (D-IL) included language similar to the SIREN Act (S. 2830, H.R. 5429) to reauthorize the Rural EMS Grant program. However, in an effort to ensure the funding would go to the most needy, small, and rural EMS providers, the language of the amendment and SIREN Act would change the eligibility to just governmental and non-profit EMS agencies. Therefore, small rural for-profit ambulance service providers would no longer be eligible to apply for grants.
The AAA is pressing Senator Durbin as well as other members supportive of the reauthorization to revise the language to ensure small rural for-profit providers would still be able to apply for grants. In the next few weeks, the AAA will be asking AAA members to reach out to their members of Congress in support of the final Farm Bill including the reauthorization language and that it continues to also apply to for-profit providers as well.
Easing Regulatory Burdens
Over the last year, the AAA has responded to several requests for information from CMS as well as Congress on how to ease regulatory burdens for Medicare providers and suppliers. In addition to these broader opportunities, representatives of the AAA and our members have been meeting with CMS officials to reduce burdens for our industry. As a specific example, we are pushing for the elimination of the PCS for interfacility transports and to expand the categories of facility personnel eligible to sign the form.
Protecting Non-Emergency Ambulance Services
The AAA continues to educate members of Congress and congressional staff about the importance of non-emergency ambulance services. We are providing congressional offices with a clearer picture as to the vital role of these transports as part of the overall health care system. We are also looking to ensure that changes in federal payor policies strengthen the role and distinction of non-emergency ambulance transports from non-medical transportation services to health care facilities.
Zip Code Changes
The current use of Rural-Urban Commuting Areas (RUCA) as the basis of the Goldsmith Modification for determining rural areas in larger urban counties needs to be reformed. There are numerous examples of zip codes that are designated as urban under the Medicare ambulance fee schedule that are clearly rural. The AAA Rural Task Force is leading the way on both short-term and long-term efforts to more accurately capture rural zip codes in large urban counties. The AAA will include the ultimate reform provision crafted by the Task Force within the Community Bill as well as look at other legislative opportunities to make the changes.
Questions?: Contact Us
If you have questions about the legislation or regulatory initiatives being undertaken by the AAA, please do not hesitate to contact a member of the AAA Government Affairs Team.
Tristan North – Senior Vice President of Government Affairs tnorth@ambulance.org | (703) 610-0216
Ruth Hazdovac – AAA Senior Manager of Federal Government Affairs rhazdovac@ambulance.org | (703) 610-5821
Aidan Camas – Manager of State & Federal Government Affairs acamas@ambulance.org | (703) 610-9039
Thank you for your continued membership and support.
CMS Issues Data Elements and Templates for Non-Emergency Ambulance Transports (NEAT): Open Door Forum for
Thursday, July 26, 2018 Just Announced
As part of its Patients Over Paperwork Project, the Centers for Medicare & Medicaid Services (CMS) Provider Compliance Group (PCG) has been hosting quarterly listening sessions and reviewing the Request for Information submissions. The American Ambulance Association has been actively engaged in these efforts, highlighting the recommendations we submitted to CMS and the House Ways & Means Committee last year. These recommendations included suggestions as to how CMS could streamline regulatory requirements to eliminate duplicative requirements and reduce regulatory burdens. In addition to these efforts, CMS has been working to standardize documentation data elements and establish templates that providers and suppliers can use to help make the current documentation processes less burdensome as well.
On July 24, CMS released draft documentation-related clinical data elements and clinical templates that could be used for the Physician Certification Statement, Progress Notes, and Prior Authorization requests. View the Documents. These documents are not intended to change current law.
CMS also announced yesterday that it will discuss the templates on a Special Open Door Forum which is scheduled for July 26 at 2-3 pm ET. The call-in information is:
Participant Dial-In Number: 1-(888)-989-4575
Conference ID: 3068545
We have shared our concern about the short notice about the call and CMS has indicated it will continue to take comments on the documents after the call as well. The AAA is in the process of reviewing these documents closely and will develop a written comment letter to provide to CMS after the call on Thursday. We welcome input from all our members as part of this process.
While these new documents may be helpful for many services, the AAA also remains committed to move its recommendations which would result in some changes in the PCS and other ambulance provider and supplier requirements.















 In honor of today’s
In honor of today’s