
CMS Proposes Modifications to Ambulance Cost Collection System
This content is for AAA members only.
Please either or Join!
Please either or Join!

Webinar July 7, 2021 | 13:00–13:30 ET | Free to AAA Members
Speakers: Kathy Lester, Esq. & Asbel Montes
On July 1, CMS issued a proposed rule on Surprise Billing which applies to those providers and physicians identified in the No Surprises Act. This statute subjected ground ambulance suppliers to an HHS Advisory Committee process prior to any rulemaking addressing these services.
The consultants and staff of the American Ambulance Association are doing a deep dive into the 400+ page rule and evaluating its nuances. We continue to understand from our conversations that ground ambulances are not included and instead are subjected to the Advisory Committee.
The American Ambulance Association will soon provide a summary to members, and will address any confusion with the Administration. Join AAA for a quick take live webinar on July 7 at 13:00 ET to learn more!

FOR IMMEDIATE RELEASE
June 21, 2021
Contact: CMS Media Relations
CMS Media Inquiries
New Medicaid and CHIP Enrollment Snapshot Shows Almost 10 million Americans Enrolled in Coverage During the COVID-19 Public Health Emergency
Report Shows Record Medicaid Enrollment and Highlights the Program’s Importance in Preserving Coverage for Millions of Children and Adults Throughout the United States
The Centers for Medicare & Medicaid Services (CMS) released a new Enrollment Trends Snapshot report today showing a record high, over 80 million individuals have health coverage through Medicaid and the Children’s Health Insurance Program (CHIP). Nearly 9.9 million individuals, a 13.9% increase, enrolled in coverage between February 2020, the month before the public health emergency (PHE) was declared, and January 2021.
Among the 50 states and the District of Columbia, a total of 80,543,351 people were enrolled and receiving full benefits from the Medicaid and CHIP programs by the end of January 2021. In the 50 states that reported total Medicaid child and CHIP enrollment data for January 2021, over 38.3 million children were enrolled in Medicaid and CHIP combined, approximately 50% of the total Medicaid and CHIP enrollment. These numbers highlight the essential role the Medicaid and CHIP programs play in providing quality and needed coverage for millions of vulnerable children and adults. In fact, both programs serve as the largest single source of health coverage in the country.
“The Biden-Harris administration is using every lever to ensure any American needing access to quality health coverage receives it. Now more than ever, people need the peace of mind of knowing that they have health coverage,” said HHS Secretary Xavier Becerra. “This report reminds us what a critical program and rock Medicaid continues to be in giving tens of millions of children and adults access to care. This pandemic taught us that now more than ever, we must work to strengthen Medicaid and make it available whenever and wherever it’s needed using the unprecedented investments Congress provided.”
The increase in total Medicaid and CHIP enrollment is largely attributed to the impact of the COVID-19 PHE, in particular, enactment of section 6008 of the Families First Coronavirus Response Act (FFCRA). FFCRA provides states with a temporary 6.2% payment increase in Federal Medical Assistance Percentage (FMAP) funding. States qualify for this enhanced funding by adhering to the Maintenance of Effort requirement, which ensures eligible people enrolled in Medicaid stay enrolled and covered during the PHE.
“Medicaid and CHIP serve as a much-needed lifeline for millions of people throughout this country. The increase we are seeing is exactly how Medicaid works: the program steps in to support people and their families when times are tough,” said CMS Administrator Chiquita Brooks-LaSure. “For the parents that may have lost a job or had another life change during the pandemic, having access to coverage for themselves and their kids is life-changing. CMS is committed to ensuring our nation’s marginalized communities and low-income families have the coverage they need.”
To assist states and territories in their response to the COVID-19 PHE, CMS developed numerous strategies to support Medicaid and CHIP programs in times of crisis, including granting states more flexibility in their Medicaid and CHIP operations. Today’s data release also reflects a range of indicators related to key application, eligibility, and enrollment processes from within state Medicaid and CHIP agencies.
The Snapshot is a product of the Centers for Medicare and Medicaid CHIP Services (CMCS) Medicaid and CHIP Coverage Learning Collaborative (MACLC), which monitors Medicaid and CHIP enrollment trends, primarily using the CMS Performance Indicator (PI) data reported to CMS by state Medicaid and CHIP agencies. PI data reflects key Medicaid and CHIP business processes- including applications, renewals, eligibility determinations, and enrollment.
The Enrollment Trends Snapshot, which is released monthly, is available here: https://www.medicaid.gov/
The complete dataset, including data from January 2021, is available on data.Medicaid.gov.

Yesterday, Senators Catherine Cortez Masto (D-NV) and Susan Collins (R-ME) introduced the Protecting Access to Ground Ambulance Medical Services Act of 2021 (S. 2037). Senators Cortez Masto and Collins were joined by Senators Debbie Stabenow (D-MI), Bill Cassidy (R-LA), Patrick Leahy (D-VT) and Bernie Sanders (D-VT) as primary cosponsors and leads on the legislation.
S. 2037 is identical to H.R. 2454 by Representatives Terri Sewell (D-AL), Devin Nunes (R-CA), Peter Welch (D-VT) and Markwayne Mullin (R-OK) and would extend the temporary Medicare ground ambulance increases of 2% urban, 3% rural and the super rural bonus payment for five years. The increases are currently scheduled to expire on December 31, 2022. The five-year extension would allow for the increases to remain in place during the two-year delay on ambulance data collection due to the COVID-19 public health emergency, an analysis of the data by MedPAC and subsequent action by the Congress to reform the Medicare ambulance fee schedule.
The legislation would also help ensure that rural zip codes in large urban counties remain rural following geographical changes under the fee schedule as a result of the 2020 census data. The current definition using rural urban commuting areas (RUCA) in Goldsmith Modification areas would be modified for zip codes with 1,000 people or less per square mile would also be rural. Ground ambulance service providers and suppliers could also petition the Centers for Medicare and Medicaid Services (CMS) to make the argument that a specific zip code should be rural. It is vital that this provision be implemented before CMS makes changes from the 2020 census data which will likely occur in 2023.
The AAA has been leading the effort on the legislation with the support of the International Association of Fire Chiefs, International Association of Fire Fighters, National Association of EMTs, National Rural Health Association and the National Volunteer Fire Council.
The AAA will be launching a Call to Action shortly requesting AAA members to ask their Senators to cosponsor S. 2037, and reach out to their Representatives to cosponsor H.R. 2454 if they have not already done so.
We greatly appreciate the leadership of Senators Cortez Masto, Collins, Stabenow, Cassidy, Leahy, and Sanders on this vitally important legislation.
Thank you @SenCortezMasto, @SenatorCollins, @SenBillCassidy, @SenStabenow, @SenatorLeahy, and @SenSanders for collaborating to support America's #EMS providers in the pandemic and beyond! #SupportEMS #AlwaysOpen #MobileHealthcare #NotJustaRide pic.twitter.com/q7Divtby8z
— AmericanAmbulanceAsc (@amerambassoc) June 10, 2021
Please either or Join!

From CMS on June 9, 2021
As part of President Biden’s commitment to increasing access to vaccinations, CMS announced an additional payment amount for administering in-home COVID-19 vaccinations to Medicare beneficiaries who have difficulty leaving their homes or are otherwise hard-to-reach. This announcement further demonstrates continued efforts of the Biden-Harris Administration to meet people where they are and make it as easy as possible for all Americans to get vaccinated. There are approximately 1.6 million adults 65 or older who may have trouble accessing COVID-19 vaccinations because they have difficulty leaving home.
While many Medicare beneficiaries can receive a COVID-19 vaccine at a retail pharmacy, their physician’s office, or a mass vaccination site, some beneficiaries have great difficulty leaving their homes or face a taxing effort getting around their communities easily to access vaccination in these settings. To better serve this group, Medicare is incentivizing providers and will pay an additional $35 per dose for COVID-19 vaccine administration in a beneficiary’s home, increasing the total payment amount for at-home vaccination from approximately $40 to approximately $75 per vaccine dose. For a two-dose vaccine, this results in a total payment of approximately $150 for the administration of both doses, or approximately $70 more than the current rate.
“CMS is committed to meeting the unique needs of Medicare consumers and their communities – particularly those who are home bound or who have trouble getting to a vaccination site. That’s why we’re acting today to expand the availability of the COVID-19 vaccine to people with Medicare at home,” said CMS Administrator Chiquita Brooks-Lasure. “We’re committed to taking action wherever barriers exist and bringing the fight against the COVID-19 pandemic to the door of older adults and other individuals covered by Medicare who still need protection.”
Delivering COVID-19 vaccination to access-challenged and hard-to-reach individuals poses some unique challenges, such as ensuring appropriate vaccine storage temperatures, handling, and administration. The CDC has outlined guidance to assist vaccinators in overcoming these challenges. This announcement now helps to address the financial burden associated with accommodating these complications.
The additional payment amount also accounts for the clinical time needed to monitor a beneficiary after the vaccine is administered, as well as the upfront costs associated with administering the vaccine safely and appropriately in a beneficiary’s home. The payment rate for administering each dose of a COVID-19 vaccine, as well as the additional in-home payment amount, will be geographically adjusted based on where the service is furnished.
As this action demonstrates, a person’s ability to leave their home should not be an obstacle to getting the COVID-19 vaccine. As states and the federal government continue to break down barriers – like where vaccines can be administered – resources for connecting communities to vaccination options remain key. Unvaccinated individuals and those looking to assist friends and family can:
The federal government is providing the COVID-19 vaccine free of charge or with no cost-sharing for all people living in the United States. As a condition of receiving free COVID-19 vaccines from the federal government, vaccine providers cannot charge patients any amount for administering the vaccine.
Because no patient can be billed for COVID-19 vaccinations, CMS and its partners have provided a variety of information online for providers vaccinating all Americans regardless of their insurance status:
The Biden-Harris Administration is providing free access to COVID-19 vaccines for every adult living in the United States. For individuals who are underinsured, providers may submit claims for reimbursement for administering the COVID-19 vaccine through the COVID-19 Coverage Assistance Fund administered by HRSA after the claim to the individual’s health plan for payment has been denied or only partially paid. Information is available at https://www.hrsa.gov/covid19-coverage-assistance.
For individuals who are uninsured, providers may submit claims for reimbursement for administering the COVID-19 vaccine to individuals without insurance through the Provider Relief Fund, administered by HRSA. Information on the COVID-19 Claims Reimbursement to Health Care Providers and Facilities for Testing, Treatment, and Vaccine Administration for the Uninsured Program is available at https://www.hrsa.gov/CovidUninsuredClaim.
More information on Medicare payment for COVID-19 vaccine administration – including a list of billing codes, payment allowances and effective dates – is available at https://www.cms.gov/medicare/covid-19/medicare-covid-19-vaccine-shot-payment.
More information regarding the CDC COVID-19 Vaccination Program Provider Requirements and how the COVID-19 vaccine is provided through that program at no cost to recipients is available at https://www.cdc.gov/vaccines/covid-19/vaccination-provider-support.html.

Please either or Join!

Please either or Join!

CMS Increases Medicare Payment for COVID-19 Vaccinations
By Brian S. Werfel, Esq.
On March 15, 2021, the Centers for Medicare and Medicaid Services (CMS) announced that it would be increasing the Medicare payment amount for administrations of the COVID-19 vaccines.
The original Medicare reimbursement rate depended, in part, on whether the vaccine being administered required a two-dose regimen (as is the case for the Pfizer-Biontech and Moderna vaccines), or a single dose (Johnson & Johnson vaccine). For vaccinations that require a two-dose regime, CMS initially paid: (1) $16.04 for the administration of the first dose and (2) $28.39 for the administration of the second dose. For vaccines that require only a single dose, Medicare paid $28.39 for the administration of that single dose.
Effective for vaccinations administered on or after March 15, 2021, CMS has increased these payments to $40 per administration. Thus, the total reimbursement for a vaccine requiring a single dose will be $40, while the total reimbursement for a vaccine requiring a two-dose regimen will be $80.

Please either or Join!

It appears that members of Congress on the House Ways & Means, Energy & Commerce, and Education & Labor Committees along with the Senate Health, Education, Labor, & Pensions Committee have reached a compromise agreement that will allow “surprise” billing legislation to be considered for passage before the end of the year. While the details of the legislation have yet to be unveiled, the American Ambulance Association has learned that it is likely to include provisions related to ground ambulance service and air ambulance service providers and suppliers.
Earlier legislation moved forward by the House Education & Labor Committee included a requirement for the Administration to create a Federal Advisory Committee to review ways to increase transparency around fees and charges for ground ambulance services and to better inform consumers about their treatment options. We believe that this language will be included in the compromise, but that there may be an opportunity to suggest modifications to make it more balanced and fairer in terms of the charge of the Committee and the types of individuals and organizations who will be selected to participate on it. The AAA is recommending that the Advisory Committee have at least a year to study and report on issues related to balance billing by ground ambulance service providers and suppliers, including the role of local and state governments in EMS systems amongst other considerations. It is also important that the Committee members include representatives from all types, sizes, and geographical areas of ground ambulance service providers and suppliers, as well as state EMS officials, and paramedics and EMTs.
It is likely that if the congressional leadership agree to move this legislation forward, it would be attached to the end of the year packages that may also include COVID-19 relief, Medicare extenders, and the annual spending bills.

Section 1834(l)(3)(B) of the Social Security Act mandates that the Medicare Ambulance Fee Schedule be updated each year to reflect inflation. This update is referred to as the “Ambulance Inflation Factor” or “AIF”.
The AIF is calculated by measuring the increase in the consumer price index for all urban consumers (CPI-U) for the 12-month period ending with June of the previous year. Starting in calendar year 2011, the change in the CPI-U is now reduced by a so-called “productivity adjustment”, which is equal to the 10-year moving average of changes in the economy-wide private nonfarm business multi-factor productivity index (MFP). The MFP reduction may result in a negative AIF for any calendar year. The resulting AIF is then added to the conversion factor used to calculate Medicare payments under the Ambulance Fee Schedule.
For the 12-month period ending in June 2020, the federal Bureau of Labor Statistics (BLS) has calculated that the CPI-U has increased by 0.646%.
Cautionary Note Regarding CPI-U. Members should be advised that the BLS’ calculations of the CPI-U are preliminary, and may be subject to later adjustment. Therefore, it is possible that these numbers may change.
CMS has yet to release its estimate for the MFP for calendar year 2021. Since its inception, this number has fluctuated between 0.3% and 1.2%. For calendar year 2020, the MFP was 0.7%. Under normal circumstances, it would be reasonable to expect the 2021 MFP to be within a percentage point or two of the 2020 MFP. However, the economic impact of the COVID-19 pandemic makes predictions on the MFP difficult at this point.
Accordingly, the AAA is not in a position to confidently project the 2021 Ambulance Inflation Factor at this point in time. However, the relative low increase in the CPI-U strongly suggests that the 2021 Ambulance Inflation Factor will be significantly lower than last year’s increase of 0.9%.
The AAA will notify members once CMS issues a transmittal setting forth the official 2021 Ambulance Inflation Factor.

American Ambulance Association Medicare Consultant Brian Werfel, Esq provides a brief update on the HHS COVID-19 Provider Relief Fund.

On July 7, 2020, CMS updated its Coronavirus Disease 2019 (COVID-19) Provider Burden Relief Frequently Asked Questions (FAQs). As part of this update, CMS indicated that it would resume several program integrity functions, starting on August 3, 2020. This includes pre-payment and post-payment medical reviews by its Medicare Administrative Contractors (MACs), the Supplemental Medical Review Contractor (SMRC), and the Recovery Audit Contractors (RACs). This also includes the resumption of the Prior Authorization Model for scheduled, repetitive non-emergency ambulance transports. These programs had been suspended by CMS in March in response to the COVID-19 pandemic.
Resumption of Medicare Fee-For-Service Medical Reviews
CMS suspended most Medicare FFS medical reviews on March 30, 2020. This included pre-payment medical reviews conducted by its MACs under the Targeted Probe and Educate program, as well as post-payment reviews by its MACs, the SMRC, and the RACs. CMS indicated that, given the importance of medical review activities to CMS’ program integrity efforts, it expects to discontinue its “enforcement discretion” beginning on August 3, 2020.
CMS indicated that providers selected for review should discuss any COVID-related hardships that might affect the provider’s ability to respond to the audit in a timely fashion with their contractor.
CMS further indicated that its contractors will be required to consider any waivers and flexibilities in place at the time of the dates of service of claims selected for future review.
Resumption of Prior Authorization Model
Under the Repetitive, Scheduled, Non-Emergent Ambulance Transport Prior Authorization Model, ground ambulance providers in affected states are required to seek and obtain prior authorization for the transportation of repetitive patients beyond the third round-trip in a 30-day period. The Prior Authorization Model is currently in place in Delaware, Maryland, New Jersey, North Carolina, Pennsylvania, South Carolina, Virginia, West Virginia, and the District of Columbia.
On March 29, 2020, CMS suspended certain claims processing requirements under the Prior Authorization Model. During this “pause,” claims for repetitive, scheduled, non-emergency transports were not be stopped for pre-payment review to the extent prior authorization had not been requested prior to the fourth round trip in a 30-day period. However, CMS continued to permit ambulance providers to submit prior authorization requests to their MACs.
CMS indicated that full model operations and pre-payment review would resume for repetitive, scheduled non-emergent ambulance transportation submitted in the model states on or after August 3, 2020. CMS stated that the MACs will be required to conduct postpayment review on claims that were subject to the model, and which were submitted and paid during the pause. CMS further indicated that it would work with the affected providers to develop a schedule for postpayment reviews that does not significantly increase the burden on providers.
CMS stated that claims that received a provision affirmation prior authorization review decision, and which were submitted with an affirmed Unique Tracking Number (UTN) will continue to be excluded from most future medical review.
As we recently reported, CMS announced that it will be delaying the implementation of the statutorily mandated ambulance data collection system. CMS has released a new set of Frequently Asked Questions (FAQs) clarifying the delay. In sum, ambulance organizations selected to provide cost data for 2020 will now be required to report 2021 data in Year 2. CMS will also add a new set of ambulance organizations for Year 2 reporting as well. This means that twice as many ambulance organizations will be reporting 2021 data in Year 2 and there will be no data reported for 2020. Any organization selected that does not report data will be subject to the 10 percent penalty, unless an exception applies. In addition to addressing concerns about reporting during the pandemic, the FAQs suggest that CMS is concerned that 2020 data “may not be reflective of typical costs and revenue associated with providing ground ambulance services.”
The complete list of these questions, as well as previous ambulance FAQs for COVID-19 on Medicare Fee-for-Service (FFS) Billing can be found here. The new data collections are below.
1. Question: CMS requires selected ground ambulance organizations to collect cost, revenue, utilization, and other information through the Medicare Ground Ambulance Data Collection System. The collected information will be provided to MedPAC, which is required to submit a report to Congress on the adequacy of Medicare payment rates for ground ambulance services and geographic variations in the cost of furnishing such services. Will the data collection and reporting requirements for the Medicare Ground Ambulance Data Collection System be delayed due to COVID-19?
Answer: Yes. CMS has issued a blanket waiver: https://www.cms.gov/files/document/summary-covid-19-emergency-declaration- waivers.pdf due to the PHE for the COVID-19 pandemic. CMS is modifying the data collection period and data reporting period, as defined at 42 CFR §414.626(a), for ground ambulance organizations that were selected by CMS to collect data beginning between January 1, 2020, and December 31, 2020 (Year 1).
Under this modification, these ground ambulance organizations can select a new data collection period that begins between January 1, 2021, and December 31, 2021; collect the necessary data during their selected data collection period; and submit the data during the data reporting period that corresponds to their selected data collection period.
CMS is modifying this data collection and reporting period to increase flexibilities for ground ambulance organizations that would otherwise be required to collect data in 2020–2021 so that they can focus on their operations in support of patient care.
As a result of this modification, ground ambulance organizations selected for year 1 data collection and reporting will collect and report data during the same period of time that will apply to ground ambulance organizations selected by CMS under §414.626(c) to collect data beginning between January 1, 2021, and December 31, 2021 (year 2) for purposes of complying with the data reporting requirements described at §414.626.
For additional information on the Medicare Ground Ambulance Data Collection System, please visit the Ambulances Services Center website at
https://www.cms.gov/Center/Provider-Type/Ambulances-Services-Center.
New: 6/16/20
2. Question: Will the 10 percent payment reduction still apply to ground ambulance organizations that are now required to collect and report data under the modified data collection and reporting period but do not sufficiently report the required data?
Answer: Yes. The 10 percent payment reduction described at 42 CFR §414.610(c)(9) will still apply if a ground ambulance organization is selected to collect and report data under the modified data collection and reporting timeframe, but does not sufficiently submit the required data according to the modified timeframe and is not granted a hardship exemption. The payment reduction will be applied to payments made under the Medicare Part B Ambulance Fee Schedule for services furnished during the calendar year that begins following the date that CMS provides written notification that the ground ambulance organization did not submit the required data.
New: 6/16/20
3. Question: The modification states that the ground ambulance organizations that were selected by CMS to collect data beginning between January 1, 2020, and December 31, 2020 (year 1) can select a new continuous 12-month data collection period that begins between January 1, 2021, and December 31, 2021. Do the ground ambulance organizations that were selected in year 1 have an option to continue with their current data collection period that started in early 2020 or choose to select a new data collection period starting in 2021?
Answer: No. The ground ambulance organizations that were selected for year 1 do not have an option and must select a new data collection period that begins in 2021. CMS cannot permit this option because the data collected in 2020 during the PHE may not be reflective of typical costs and revenue associated with providing ground ambulance services. New: 6/16/20
4. Question: Does the guidance mean that there will be no data reporting in 2021 and that both the ground ambulance organizations that were selected for year 1 and the ground ambulance organizations that will be selected for year 2 will collect and report data during the same time periods?
Answer: Yes. Under the modification, ground ambulance organizations that are selected for year 1 will not collect data in 2020. These ground ambulance organizations will select a new data collection period that begins in 2021 and must submit a completed Medicare Ground Ambulance Data Collection Instrument during the data reporting period that corresponds to their selected data collection period. As a result of the modification, year 1 and year 2 selected ground ambulance organizations will collect and report data during the same time periods. New: 6/16/20
CMS has issued a blanket waiver modifying the data collection period for the ground ambulance services that were selected to report in Year 1. Under the current law, these organizations would have been required to collect data beginning January 1, 2020, and through December 31, 2020. The waiver allows these organizations to select a new continuous 12-month data collection period that begins between January 1, 2021 and ends December 31, 2021. This modification means that such organizations will collect and report data during the same time period as the ground organizations that CMS will select for Year 2 of the cost collection program.
From the summary of the waiver, it appears that organizations will have the choice of submitting data in Year 1 or Year 2. CMS has not moved the timeline for any other data collection year, so there is the potential for a substantial number of organizations to report in Year 2, which would increase the amount of data available.
The AAA has supported the data collection system to make sure that CMS and the Congress have valid and reliable data to support maintaining the geographic add-ons to the Medicare Ambulance Fee Schedule and to support efforts to address the chronic underfunding of the Medicare Ambulance Fee Schedule.
The complete FAQ is below and also available at: https://www.cms.gov/files/document/summary-covid-19-emergency-declaration-waivers.pdf (on page 29).
“CMS is modifying the data collection period and data reporting period, as defined at 42 CFR § 414.626(a), for ground ambulance organizations (as defined at 42 CFR § 414.605) that were selected by CMS under 42 CFR § 414.626(c) to collect data beginning between January 1, 2020 and December 31, 2020 (year 1) for purposes of complying with the data reporting requirements described at 42 CFR § 414.626. Under this modification, these ground ambulance organizations can select a new continuous 12-month data collection period that begins between January 1, 2021 and December 31, 2021, collect data necessary to complete the Medicare Ground Ambulance Data Collection Instrument during their selected data collection period, and submit a completed Medicare Ground Ambulance Data Collection Instrument during the data reporting period that corresponds to their selected data collection period. CMS is modifying this data collection and reporting period to increase flexibilities for ground ambulance organizations that would otherwise be required to collect data in 2020- 2021 so that they can focus on their operations and patient care.”
“As a result of this modification, ground ambulance organizations selected for year 1 data collection and reporting will collect and report data during the same period of time that will apply to ground ambulance organizations selected by CMS under 42 CFR § 414.626(c) to collect data beginning between January 1, 2021 and December 31, 2021 (year 2) for purposes of complying with the data reporting requirements described at 42 CFR § 414.626.”

On May 1, 2020, CMS updated its “COVID-19 Frequently Asked Questions (FAQs) on Medicare Fee-for-Service (FFS) Billing.” The full document can be viewed by clicking here.
In the updated FAQ, CMS answers three important questions related to ambulance vehicle and staffing requirements:
The Department of Health and Human Services recently updated its guidance on the disbursement of provider relief funds under the CARES Act for the testing and treatment of the uninsured. Previously, HHS indicated that this allocation was only available for the reimbursement of emergency and non-emergency ground ambulance transportation. However, in its most recent update, HHS has removed the restriction that limited participation to ground ambulance providers and suppliers. The new guidance indicates that the relief funds are now available for all emergency ambulance transportation and non-emergency patient transfers via ambulance.
Thus, it appears that air and water ambulance providers and suppliers are now eligible to receive funding for the treatment of COVID-19 patients.
Is there anything my air or water ambulance organization needs to do to claim reimbursement for treatment of uninsured COVID patients?
Yes. In order to be eligible for payments for the treatment of uninsured COVID patients, you must enroll as a participant in the program. Enrollment must be done through an online portal that can be accessed at: http://www.coviduninsuredclaim.hrsa.gov.
Once my organization enrolls, when can we start submitting claims for reimbursement for treatment of uninsured COVID patients?
HHS has indicated that it will begin to accept claims for reimbursement for treatment of the uninsured on May 6, 2020.
FUNDING FOR TREATMENT OF UNINSURED COVID PATIENTS IS SUBJECTED TO AVAILABLE FUNDING, AND IS THEREFORE ON A FIRST-COME, FIRST-SERVED BASIS. IT IS EXPECTED THAT THESE FUNDS WILL BE EXHAUSTED IN FAIRLY SHORT ORDER.

Use the American Ambulance Association’s simple form to estimate relief you may receive from the second tranche of HHS COVID-19 funding. Please note that not all providers will receive funds.
More information about this program as well as access to the form you must complete in the General Allocation Portal can be found on the HHS website.
For-profit and non-profit non-governmental providers, to determine your Net Patient Revenue for the portal, use the following information from your most recently filed tax return. (2019 if filed, otherwise use 2018 numbers).
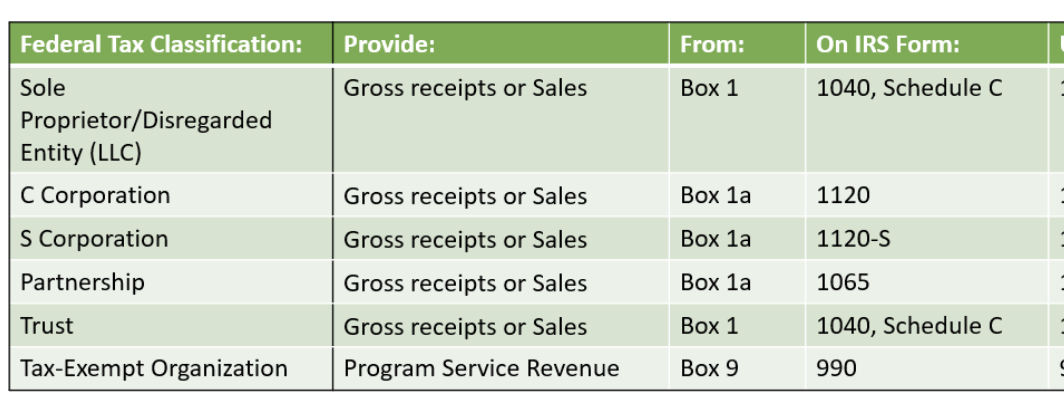
Governmental providers, enter your revenue generated for the last audited financial year. When completing the form in the portal, select Tax Exempt Organization. When asked to upload a return at the end, upload your most recent audited financials.
Please do not enter commas or dollar signs. A negative number or zero in the Tranche 2 box indicates that you WILL NOT receive funding in tranche 2.

Updated April 24, 2020 at 9:40 pm | Register for AAA’s 4/27 webinar on this topic►

At 5 p.m. on Friday, April 24, 2020, the Department of Health and Human Services opened the online portal that health care providers and suppliers must use to submit their revenue information. This is a requirement to access the second $20 billion tranche of general allocation funding. Access the online portal►
In order to provide the required information, you will need the following information/documentation:
The portal will ask a series of questions to verify your identity and the identity of your organization. These include providing your TIN and the last six digits of the bank account to which the original tranche of relief funding was provided.
After completing the verification process, you will be asked to complete an attestation that you received the initial tranche of relief funding.
You will then be prompted to complete a short questionnaire that is used to apply for additional funding. The steps for completing that questionnaire are as follows:
AAA is aware of an issue that may affect governmental EMS organizations. Specifically, those governmental agencies that do not file federal tax returns may not be able to complete the final stage of the application, which asks you to upload a copy of your most recent tax return. The AAA has reached out to HHS to request guidance on how governmental organizations should complete the form. We will update our members as soon as we know anything different. Register for our May 4 COVID-19 Financial Resources for Governmental Providers webinar►
HHS indicated that it will allocate an undisclosed portion of the $29.6 billion in otherwise unallocated relief funding to reimburse healthcare providers and suppliers for COVID-related treatment of the uninsured. Please note that this allocation is only available for the reimbursement of emergency and non-emergency ground ambulance transports. Reimbursement will be available for COVID-related care furnished with dates of service on or after February 4, 2020. Payments will be made at the Medicare rates, subject to available funding. As a condition to receipt of funding, you must agree to accept HHS’ payment as payment-in-full, i.e., you may not balance bill the uninsured patient.
Yes. In order to be eligible for payments for the treatment of uninsured COVID patients, must enroll as a participant in the program. Enrollment must be done through an online portal that will open starting on April 27, 2020. Once open, the portal can be accessed at http://www.coviduninsuredclaim.hrsa.gov.
HHS has indicated that it will begin to accept claims for reimbursement for the treatment of the uninsured at some point in early May 2020.
FUNDING FOR TREATMENT OF UNINSURED COVID PATIENTS IS SUBJECTED TO AVAILABLE FUNDING, AND IS THEREFORE ON A FIRST-COME, FIRST-SERVED BASIS. IT IS EXPECTED THAT THESE FUNDS WILL BE EXHAUSTED IN FAIRLY SHORT ORDER.
The AAA strongly recommends that all members complete their enrollment form as soon as reasonably practicable, so that you are in a position to submit claims as soon as the claim submission window opens.