May 22 at 2:20 PM | EMS1 | By AAA Communications Chair Rob Lawrence
In my last EMS One-stop column, I commented on the legislative to-do list to ensure that EMS receives the federal support it deserves right now as we staff the front lines and perhaps brace ourselves for COVID-19 round two as the nation craves a return to the normality and liberty enjoyed before the lockdown.
On May 15, 2020, the much talked about HEROES Act narrowly passed from the U.S. House of Representatives by a 208 to 199 vote to the Republican-controlled Senate. The HEROES Act proposed $3 trillion in tax cuts and spending to address the negative health and financial impacts of the COVID-19 pandemic. This included benefits for the public safety community, extensions to enhanced unemployment benefits, debt collection relief, direct cash payments to households and possibly even hazard pay.
I recently reported on how the leaders of a few of our national associations united to tell the story of EMS on the front lines and to draw attention to the shortfalls we are all encountering daily from PPE to funding. EMS providers of all denominations are also coming together at a state level to tell their story and appeal for assistance and funding to ensure the continuity of operations. On Apr. 15, 2020, the Professional Ambulance Association of Wisconsin, Wisconsin EMS Association, Professional Fire Fighters of Wisconsin, and Wisconsin State Fire Chiefs Association conducted an online press conference to discuss the mobile healthcare situation in Wisconsin.
The transcript below was lightly edited for clarity.
Amanda Riordan: Thank you for joining us today. My name is Amanda Riordan, and I am the vice president of member services for the American Ambulance Association. I’m also the administrator for the Professional Ambulance Association of Wisconsin. I’m so happy to have the opportunity to interview John Eich, the director of the Wisconsin Office of Rural Health. John is an exceptional contributor to rural health in Wisconsin. He’s also a sterling advocate for the power of EMS to assist with public health in the least accessible areas of Wisconsin. I’ll ask John a couple of questions today about the recent Rural EMS Listening Sessions that he conducted in a number of areas across the state. John, thanks again for joining us. Would you mind telling me a little bit about your background and how you became the director of the Wisconsin Office of Rural Health?
John Eich: I appreciate your inviting me to talk about some of our programs, so thank you. I took a bit of a wandering path: I’ve done everything from carpentry and marketing to social work with homeless teens. I found my way to community [service] down in southern New Mexico. I caught the bug there working on behalf of the community and society at large. When I moved back home up to Wisconsin—I grew up in a rural area here in southern Wisconsin—I saw an opening and at the Office of Rural Health. I’ve been on board ever since, and it’s a lot of fun.
Amanda Riordan: Thanks so much. And we’re so glad you took the position. Would you mind sharing a little bit about why EMS is so important to rural health?
John Eich: If you’re not familiar with an office of rural health, we receive mostly federal funding to work on the state level. There’s an office in every state in the nation. Here in Wisconsin, we are funded mostly, I would say, to work with rural hospitals and EMS, and we find that EMS is one of the areas of greatest need. Every piece of the healthcare delivery system has its challenges and its strengths. EMS, I think by the nature of having formed itself—at least rural EMS formed itself—around the model of volunteer services. In my estimation, it has sort of painted itself into a corner. It started when medicine was not as complicated, and when populations, were not expecting as much. You were helping out your neighbors by getting somebody to a hospital. It has since evolved in a good way.
[EMS has] evolved into a healthcare profession. And so there are a lot more demands. There’s a lot more education; continuing education, learning new techniques that are lifesaving. Society depends on it. But that means that these volunteer services that started off small are under increasing pressure. That’s why we are trying to dedicate as many of our resources as we can to helping out that system within Wisconsin, and it’s paying great dividends. We’ve always really enjoyed our interactions with EMS. I think it takes a particular kind of person to do it. We just really enjoy our time with those who do the work. That led us to doing what we’re calling a “Rural EMS Listening Session.” So we did five of these sessions around the state in rural areas, and we intend to do a few more.
Part of the idea was that so often policy in general happens in urban centers. In EMS policy, because the state capital is down in the very southern part of the state and Milwaukee, the largest city is also down in the southern part of the state, the rural areas of the state (which most of the rest of it) tend to feel ignored or unheard. It’s much harder for them to participate. So if somebody has to drive five hours to go to a meeting that would take [a city resident] 15 minutes to drive to, that’s a disparity in access and it’s a disparity in having your voice heard. So we decided that it was important to go listening where rural EMS is practicing. So we did that, and are continuing to do so.
It’s been very eye opening. Obviously there was a lot that we expected to hear that we did hear. I mean, there’s, there’s not a lot new here. People in EMS know what the issue is as someone said these are the same ideas we’ve been talking about for the last 20 years or more. And that’s very true. We like to believe that it’s time for things to change. We’ve been talking about this long enough. Maybe we should do our best to push the issues forward. And that’s phase two of these listening sessions: take what we heard and get it into the hands of advocates, like the EMS associations, fire associations, et cetera, and other advocates like the Office of Rural Health that try to speak on behalf of the needs of EMS. I do think I’m optimistic that legislators want to help. When they’ve been presented with bills, they’re interested. Money is always an issue, but I would say that they definitely want to be part of a solution. So, it’s all of our jobs to make sure that they have the right solutions and presented to them.
Amanda Riordan: I think that’s a great segue to one of your other very popular innovative programs in Wisconsin. The Office of Rural Health actually helped put together the EMS at the Capital Day event in 2017. Would you mind telling us a little bit more about what that entailed and the groups that participated?
John Eich: Absolutely. So again, as we work with all parts of the healthcare delivery system, we work with hospitals and clinics and providers; physicians, PAs/physician assistants, nurse practitioners, the nurses that staff the hospitals and clinics and home health services. When we look at EMS, it always strikes me how it has a level of splintering that I don’t see in other professions. In other professions, they’ve managed to sort of circle the wagons and get on the same page and present a united face to push forward their vision and their legislative goals. EMS, for whatever reason. I’m not sure why it seems to have done the work but also, identified a number of differences. You can be a paid or career staffer versus a volunteer. You can work in a rural service versus an urban. You can be in fire versus EMS. You could be a Paramedic or you could be a Basic EMT or an Emergency Medical Responder. Each of those areas, each of those groups, sort of huddle and identify amongst themselves. I would like to see them working more cohesively together and I’m sure they would as well.
The effort that that led to an EMS Day at the Capital was to try and get all of the disparate groups together and on the same page. All of them had been working very diligently on the issues that were important to them, and I think there is a lot of overlap. As one of the participants said, “We can agree on a 80 percent of the issues, we may disagree about the 20 percent, but let’s work on the 80 percent and when we get that done, then we can disagree about the rest of them.”
So that was the goal that brought the groups together. So we were lucky to be able to get the two EMS associations in the state, the state fire chiefs, and the professional firefighters. The state EMS board joined in with us as well as they could, in more of a listening capacity. We created a wish list of legislative issues and a lot of it was centered around education: who we are and what we do. And we took that to the state capital. We had tremendous turnout and we had uniforms marching through the, through the offices of the legislature both in the Assembly and the Senate. I like to think we got their attention and we plan to, as I said, take what we’re learning from this rural EMS tour, connect with our urban allies as well, and get EMS advocacy on the same page so that they can do tremendous work together.
Amanda Riordan: It was truly exciting and a privilege to witness everything that happened in November 2017 when the Professional Ambulance Association of Wisconsin, Wisconsin State Fire Chiefs Association, the Professional Firefighters of Wisconsin, and the Wisconsin EMS Association, all came together with the help of your office, the Office of Rural Health, to speak with one voice when meeting with state legislators. I think that by working together they were able to present such an incredibly compelling message to legislators and to key staff that worked with legislators. I think a lot of times people are somewhat unaware that winning over the hearts and minds of critical legislative staff is almost as important as running to over the hearts and minds of legislators themselves.
With that in mind, and with all of the successes you’ve had helping execute your vision of moving EMS and rural health forward in Wisconsin, would you mind telling us a little bit about where you see the future of rural health going in your state, Wisconsin, as well as the country in general?
John Eich: I take it you mean in EMS terms. Because there’s a lot going on in healthcare, as you know! As far as EMS goes, I think the future of EMS care is not a wholly volunteer model. I think it is at least a hybrid model, and I think the industry needs to figure out how to make that transition. I think that’s going to be a difficult and painful transition. I think it’s going to take a lot of education to the local politicians who are used to having their services and frankly to be getting a pretty good deal.
We talked recently to a small community. It was a countywide meeting, but it was held in a small community that had been [served by] a volunteer service. They said they had a core group of about five people. The chief of the service had had volunteered 4,280 hours last year. The rest of his staff [had volunteered] around the 3000-hour level. They were proud of that, understandably. They were also somewhat reluctant to consider another model in their mind. They felt that they were just fine. When I look at that from the outside, I think, “What if one of you tears an ACL as you’re getting off the ambulance rig, what if two of you get the flu really bad? Which happens!” [What happens if] then there are two calls for EMS, at the same time, while two of your staff are bedridden. That’s three people to make all those calls. I struggle with the vision of that is as sustainable.
But when the local community looked at the numbers, they said, well, it looks like as far as the taxes go, that’s about $12 per capita. I was a little horrified, and asked “is that per year?” And they said, “Oh yeah, yeah, that’s per year.” I was struck by the fact that I pay more for Netflix per month than these folks pay per year to have two highly trained individuals show up with the latest technology to save the lives of their loved ones. I’m not criticizing that, but I do think there’s an opportunity there to really examine that in the daylight. And certainly when the board realized that and looked at it, there was a lot of sort of a flurry of questions back and forth. And is this true? On and on.
I think the nature [of the matter is that] if you can possibly put the question to a citizen in a grocery store as they’re walking out with their groceries, “How much would you pay per year in your taxes to have this kind of lifesaving service?” I don’t think the answer would be $12 a year. I think it would be more, but I don’t think most citizens or politicians have been given the opportunity to really look at. I think they assume it’s already paid for. It’s part of their taxes. I think they assume that Paramedics just show up at their door. They don’t necessarily know the difference between a Paramedic and a Basic EMT or EMR. They have a great deal of faith and trust in these people, as they should. I think they’re just not aware—they’re not aware of the challenges and the lack of funding and the way the system is sort of precariously balanced on top of volunteer hours to an incredible amount. I think the future in my mind, if you look at the data and volunteerism trending down, it’s trending down across all sectors, but that is hitting EMS very hard.
If you look at staffing, we’re seeing with low unemployment that means that it’s harder and harder to fill positions. That especially happens in rural areas. People are moving to urban areas for jobs. There’s not as many people there. If they do still live in the rural area, they tend to work in a neighboring larger town or other towns, so it’s harder for them to volunteer. So I just think the data is pretty clear where we’re headed. We just culturally have to try and do some heavy lifting and change the perceptions of what a society should pay for. As Dana Sechler from the Professional Ambulance Association of Wisconsin often says, we pay for garbage collection at $138, the median per capita cost per year. Like I said, some [areas are paying just] $12 per year for EMS. Garbage is very important. I don’t mean to dismiss it, but I think we can do better for lifesavers. I see that as the primary issue.
Garbage is very important. I don’t mean to dismiss it, but I think we can do better for lifesavers. I see that as kind of the primary issue. I think another issue is certainly something we’re hearing that is in rural areas, you have a lot of Emergency Medical Responders (EMRs). They’re taking a class that is 80 hours [in duration] because they want to help their neighbors. They’re not transporting— they are showing up to be of help. But they’re taking the National Registry tests in Wisconsin, and the National Registry tests, for a lot of good reasons, is lifting the industry into a level of professionalism and knowledge that is important and necessary. But I think that certainly what we heard is that an EMR is sort of an entry level to this.
So how can we figure out a way to lower the barriers to participation, without lowering the standards of care? That’s something we need to look at. And I think frankly, as a nation, we need to look at that and have that conversation with the National Registry. I think they’re doing the work that they do, and, and in a lot of ways it’s good work, but I think they need to have feedback from their customers and all of us states are their customers. All of us need to maintain a dialogue with them and say, this is what we need. We may need critical thinking in our clinicians, but do we need it in our technicians? Do we need it in our EMRs? [For EMRs] do we need sort of tricky questions that two of them are correct and you have to sort of guess which correct answer you wanted to give? I think it’s that sort of stuff that demoralizes local people who may not be eager to take a test in the first place and are a little put off by a computerized test in the second place. Then if they don’t pass, they go right back home to their church, their gas station, and their bar and tell everybody how this impossible test is not worth their time. I’m not against the National Registry tests, but I do think that we need to have more conversation about it and we need to find ways to lower the barriers and maybe that’s preparing EMRs in a different way.
I’ve got a daughter who is preparing for the ACT [college entrance test], and she’s learning the tips and tricks. She’s in a class just to help her take that test, and a lot of it’s not even about the content. Maybe since the National Registry is modeled on these other types of tests we need to train more on not necessarily the skill levels of how to save someone’s life, but how to take a test, which seems a little weird. But if that is our standard, then we need to make sure that our people are prepared when they walk into that room.
Amanda Riordan: That makes a lot of sense. Certainly we hear feedback in both directions from a variety of different stakeholders regarding the increasing professionalization of EMS. On one end, of course, we want to honor and maintain the contributions of those mission critical volunteer providers, particularly in rural areas, and on the other hand we have the push-pull of a Paramedic, in particular, looking for additional certifications and additional recognition of mobile health care as a profession. All of that mixed together with a flat or diminishing reimbursement makes sustaining a mobile healthcare/EMS in all areas really challenging. But of course as you so aptly pointed out, it especially impactful areas of our country and in a state like Wisconsin where you have so much land mass that is in rural areas. [These issues] particularly impact states of that nature is as they look forward to an aging population and the movement of younger people into urban areas. So truly appreciate those insights and those suggestions. And it’s certainly something that I’m sure there will be continued dialogue about for years to come.
John Eich: And I would like to say that I see a real difference between a Paramedic—or in Wisconsin, we also have the Advanced EMT classification—where we are expecting them to have a body of knowledge and to be healthcare clinicians, to be making life or death decisions in the field. Absolutely. Everyone in society wants those people to be the best-trained, the most knowledgeable, at the top of their game. And the tests should reflect that. I do think that if we have someone who is a firefighter who’s driving out to a site to assist, that’s not the same as a Paramedic and I’m not saying that they shouldn’t be trained and there shouldn’t be a gates for them to go through. We need to be sure that they are trained to the best of their scope and to the best of their ability. But I think it’s a different level of care is a different kind of professionalism. So I think we just need to really make sure that we’re doing a service to the rural areas where they are scraping together five people to cover a very large area and they just don’t have time for the level of nuance that you will often see in an urban, metro area where you’ve got, um, you’ve got enough staff to cover these sort of things,
Amanda Riordan: Makes complete sense and certainly something that we know so many communities are wrestling with right now. I thank you for bringing it to everyone’s attention. I think that we will get some lively dialogue in the comments when we get this posted about, as you pointed out, the diminishing volunteerism as well as the other pressures facing most mobile healthcare these days. Before we wrap up here, would you mind giving us some tips or thoughts about how EMS providers, mobile healthcare providers, in Wisconsin can work best with your office? Or if you have any generalized tips about how ambulance services and fire departments across the country can best work with the Offices of Rural Health in their state, we would be very grateful. Clearly you are moving and shaking in Wisconsin and we’d love to see that ripple out to other states.
John Eich: Absolutely. So, I have counterparts in every state and they’re all doing great work when it comes to rural health and rural EMS. If someone in any state simply goes to Google and, enters their state name and “office of rural health,” they’ll get right to them. I think there is a difference between Offices of Rural Health. Many of us are in state government, and so what you experienced there is common of state government—It’s a more bureaucratic system. The websites tend to be a little bit trickier to find the information because there’s obviously a lot going on there and some political considerations. We [here in Wisconsin] are university-based. There’s about 12 of those around the nation, and three that are nonprofit, so, even leaner and more flexible. So every [office] will look differently.
I do think that EMS should reach out to their Offices of Rural Health to let them know about their needs, because when we look at metrics for healthcare and for population health, we see the metrics getting worse. It’s almost like a horseshoe in that they get worse the more rural and remote you are. Suburban areas have the lowest need, and then the inner city tends to be equally challenging. We share a lot of population health issues with inner cities. The difference I think is really transportation. We’re farther away. And if you don’t have a car, you’re really isolated and stuck, so EMS is mission critical.
If you think about that first hour of care being so important to outcomes, [if sick or injured in a rural area] your first half hour could be without care as people are getting to you and you’re trying to find a cell signal to actually call 911. Once they arrive, your rural EMS providers are the people that are giving you that care. So it is vitally important that those people have the resources to do their job the best that they can.
Please reach out to express your needs. One of the things we’ve been talking about based on this Rural Listening Tour and talking with our state EMS office and the associations just yesterday is the idea of some kind of helpline; Somebody to answer the call when a service is identifying that they are really struggling, because [rural services] are a little nervous about calling the state and saying, “Hey, guess what? Things are really rough here. You might want to shut us down.” Nobody wants that. The state EMS office is very clear that it’s not in anybody’s best interest to remove care and burden neighboring services. So getting a helpline with a number of resources and even someone that can drive out and sit across the table and talk through some issues and get some advice would be very helpful for some of these services that are really struggling. Those are some ways that I think folks can get involved, and I’m always interested in hearing more.
Amanda Riordan: John, thank you so very much for your time and insights today. It has been an absolute pleasure talking to you and I’m sure that we’ll be hearing a lot more from the Office of Rural Health, you, and your staff in the years to come. So again, we truly appreciate it and wish you a very happy National Rural Health Day tomorrow, November 15th.
John Eich: Thank you very much, and I look forward to celebrations around the nation.
Congratulations! You were selected for the Paramedic Supervisor position, if you accept, we’ll start the transition immediately.
I remember the excitement I had when I heard those words so many years ago. The excitement that carried strongly through 2 days of celebrating with my husband, anticipating the new world I was about to be part of; making a mental list of all the mountains I couldn’t wait to move! This excitement was quickly drowned by a sinking feeling deep in my gut. It felt like running out of gas on a country highway at one in the morning and your cell phone is dead; it’s dark, there is nobody around, and you cannot phone a friend.
Whether it comes right away, or later—because of the reaction of people we thought were friends or feeling overwhelmed in a new situation you were expected to handle with precision, we’ve all felt that feeling as a new leader. By sharing our stories with one another, the success and the failures, we all grow.
I remember getting so much advice from those who walked the road before me, some solicited some not. The stories were sometimes shocking, often comical and always gave me perspective and insight into my own blunders – most importantly the stories many shared with me taught me the importance of humility and the ability to laugh at myself, admit my mistakes, learn and move on. At some point, the tide started turning, and friends and colleagues began asking me for my stories and advice. Although I often felt like I wasn’t experienced (i.e. old enough) to be offering any advice I realized it’s not necessarily the age or years of experience behind the story that makes it meaningful. The power is in the ability to share an experience through storytelling—finding common ground amongst the hierarchy of titles and job descriptions.
I think it is easy to lose sight of how our words and actions can affect others as we are wrapped up in our day to day and moving down the checklist of tasks. The influence of a leader in an organization, even an informal leader, is long lasting and not to be taken for granted. Over the past year, I’ve been talking to many EMS leaders of the past and present. I’ve been asking them what they wish they would have known when they first started their leadership journey, and what advice they might give to others just starting out. Here are 10 of the most common answers I received.
Top 10 Things I Wish I Had Known
I wish I would have known I could be myself. Being myself earned me the role, but suddenly it didn’t seem like enough. At first, I thought others were putting all this pressure on me to be an amazing supervisor immediately – in hindsight, I realize I was putting the pressure on myself and it was totally unnecessary. Being myself allowed me to be a more effective supervisor for my team and I wish it hadn’t taken me so long to figure it out.
I wish I would have learned earlier how important listening is. Listening to understand your people, listening to learn and listening to understand the politics that are happening beyond the surface.
I wish I would have known that I didn’t have to be right all the time; I wasn’t expected to be right all the time. I was only expected to be an honest and reliable resource for my team.
Change is slow. PAINFULLY slow. In EMS there is constant instant gratification – you see a problem with a patient, you fix it, you drop them off. Transitioning to an administrative role and learning that change is slow and takes time (SO MUCH TIME!) is more difficult than I ever would have imagined. I had to really learn to see the long game.
It’s not a “day job”. As a leader, you’re never off duty. Whether you’re on a regular rotation as a shift supervisor, or in the office as a manager or director, EMS is a 24/7 world which means you work nights, weekends and holidays right along with your team. You may not be on a truck or at a station—but you’re still available to them all the time.
I wish I would have understood how important mission, vision, and values really are to a company, and how important it is to talk about them with staff.
We’re all learning, and it is OK to ask for help.
Just because a staff member is asking me a question, it does not mean they are challenging my authority. As a leader, it took me a long time to realize that I should embrace a staff member challenging a decision so long as they are doing it in a constructive manner.
I wish I would have known how much of an impact I have on people. I don’t mean that in an arrogant way. I’ve had staff bring up conversations we had years ago, and I had forgotten all about it—but they were still carrying that encounter with them.
That it wasn’t for me. I thought I wanted to be a supervisor – a leader. I was wrong. I was unhappy with the role and everyone knew it but me, and I was becoming destructive.
When I came to the realization that I wasn’t the right person for the role, my boss allowed me a front row seat to the best example of leadership I have personally witnessed. He allowed me to step back from the role but didn’t forget about me; he continued to invest in me as an employee and as an individual despite the certain protest of others. To this day, he continues to provide guidance on my professional endeavors and is someone I truly look to for honest advice.
Podcasts are a great way to gain information and insight on a variety of topics. With the intimidating number of podcasts on the topic of EMS and leadership available, it can take a bit of time to find the one that’s right for you. I have been a fan of podcasts for several years now, and while some of my favorites have dropped off over the years, I am certain there are many new favorites out there waiting to be discovered.
If you’re not yet listening to podcasts, I encourage you to start exploring – here is a quick list of some of my current favorites in EMS and leadership to get you started. (* We’ve included links are iTunes, but these podcasts can be found on just about any podcast service.)
Prehospital Emergency Care Podcast
This is a newer podcast, and quickly landed on my subscribed list for the obvious reason; it is the official podcast for the NAEMSP. The first few episodes were recorded during the most recent NAEMSP annual meeting, in the most recent the hosts spend time interviewing authors of studies published in the PEC journal, discussing results questioning when, and how, changes should be implemented based on those results. I’ve been able to make the NAEMSP conference a few times, and it is truly enjoyable. This podcast is a nice way to keep up on the research and recommendations coming from the NAEMSP.
EMJ Podcast
This podcast discusses the research published in the Emergency Medicine Journal (EMJ) and is a great listen, in my opinion. The hosts are easy to listen to and the way they discuss the research and potential application is thought provoking, particularly given the international perspective.
CPR Podcast
This podcast is a little bit of everything in EMS. While most of the episodes seem to have a clinical education spin, others delve into some standard practice, leadership, and provider health and safety topics as well. The conversations are well planned without seeming overly rehearsed which ads a measure of sincerity to the commentary.
Dear HBR This is a newer podcast and is produced by the Harvard Business Review. While not directly related to EMS, there is value for EMS listeners. Individuals write to the show and ask questions – many of which are about how to handle conflicts or difficult situations in the workplace – and the hosts discuss the question at hand and the advice they might give the individual based on personal experience and available research. There is so much we can learn through the experience of others, and this is a good way to compare our own experience with the experience of others, and perhaps walk away with some good advice.
EM Weekly
This focus of this podcast is emergency management (EM), but the discussion topics span everything from tactical planning to leadership and future possibilities. The host and guests mix in a bit of the history of EM throughout the episodes which helps provide perspective and understanding of the evolution of emergency management over time, and ideas for the future.
La Crosse, WI– The American Ambulance Association (AAA), Minnesota Ambulance Association (MAA), and Professional Ambulance Association of Wisconsin (PAAW) today officially announced the launch of the Midwest EMS Expo conference and trade show. This event will take place annually in La Crosse, Wisconsin beginning in May 2018, and will feature content from national- and state-level ambulance experts.
“AAA is proud to partner with PAAW and MAA in the development of the Midwest EMS Expo. We look forward to bringing together the best in ambulance expertise to deliver a powerful educational experience for EMS leaders,” said American Ambulance Association President Mark Postma.
The program will open on Wednesday, May 2, with key updates from the American Ambulance Association’s renowned experts on EMS reimbursement and advocacy. Highlights include a federal legislative overview by AAA President Mark Postma, as well as strategies for maximizing revenue from reimbursement gurus Asbel Montes, Brian Werfel, Brian Choate, and Scott Moore.
Thursday, May 3rd’s programming was developed collaboratively by the Minnesota Ambulance Association and Professional Ambulance Association of Wisconsin. The day will begin with speaker Captain Ray Dupuis of the Watertown Police Department. In this riveting keynote, he will share what happened in first minutes after the explosions at the marathon finish line, then explain police and EMS action plans that day. Don’t miss this opportunity to learn from a seasoned public servant who helped to lead his city in its darkest hour.
Additional conference topics include employee recruitment and retention, billing and compliance, executive leadership, community paramedicine, employment law, managing across generations, EMS resilience, and many more. For a complete conference agenda, visit www.midwestemsexpo.com/schedule.
According to PAAW President Dana Sechler, “The Midwest EMS Expo will offer a platform for the exchange of ideas and information among ambulance leaders of all levels. Given the constantly changing nature of EMS, it is critical to bring this educational and networking opportunity to our region.”
In addition to powerful educational content, the Midwest EMS Expo will offer attendees the opportunity to experience the best in products, services, and vehicles for EMS providers. Gold Sponsor Savvik Buying Group will be joined by Silver Sponsor Cindy Elbert Insurance Services, Bronze Sponsor eCore, and dozens more exhibitors on the show floor. For a complete list of current vendors, please visit www.midwestemsexpo.com/exhibitors.
Conference registration is now open, with member early-bird rates as low as $200 per attendee. Sponsorship, booths, and vehicle spaces are also available online at low introductory rates. To register for the Midwest EMS Expo or view the complete schedule of events, please visit www.midwestemsexpo.com.
# # #
About the American Ambulance Association
Founded in 1979, the AAA represents hundreds of ambulance services across the United States that participate in emergency and nonemergency care and medical transportation. The Association serves as a voice and clearinghouse for ambulance services, and views prehospital care not only as a public service, but also as an essential part of the total public health care system. www.ambulance.org
About the Minnesota Ambulance Association
The Minnesota Ambulance Association represents Minnesota’s EMS providers by working with and monitoring legislation that impacts EMS, recruitment & retention, financial issues, education & leadership. We work closely with our peers in the hospitals, fire service, police, emergency managers, sheriffs & other associations. www.mnems.org
About the Professional Ambulance Association of Wisconsin
The Professional Ambulance Association of Wisconsin (PAAW) was founded in 2005 to represent the interests of ambulance services in the state of Wisconsin. In addition, PAAW works to create and promote opportunities for collaboration and networking between ambulance service executives, directors, and managers. PAAW serves as an EMS stakeholder group to promote excellence and quality in the ambulance industry in Wisconsin. www.paaw.us
2015 Medicare Payment Data Offers Evidence of Nationwide Crackdown on Non-Emergency Ground Ambulance Transportation; Impact Varies Dramatically by Medicare Administrative Contractor
Every year, CMS releases data on aggregate Medicare payments for the preceding year. This file is referred to as the Physician/Supplier Procedure Master File (PSP Master File). This past month, CMS released the 2016 PSP Master File, which contains information on all Part B and DME claims processed through the Medicare Common Working File with 2015 dates of service.
In September’s blog post, I discussed the results of the first year of the prior authorization demonstration project for repetitive, scheduled non-emergency ground ambulance transports. During this first year, the project was limited to three states: New Jersey, Pennsylvania, and South Carolina. The data confirms that these three states saw a dramatic reduction in Medicare’s approved payments for dialysis transports.
This month, I will be discussing the national payment trends for non-emergency ground ambulance transports, and, in particular, Basic Life Support non-emergencies.
In 2015, Medicare paid approximately $990 million for BLS non-emergency transports. This is 13% less than what it paid for BLS non-emergency transports in 2014 ($1.14 billion). Please note that these figures only reflect payments for the base rate; when the payments for the associated mileage are included, the reduction is even more dramatic.
In actual terms, this means Medicare Administrative Contractors (MACs) approved nearly 1 million fewer BLS non-emergency transports in 2015 (5.86 million) than they approved in 2014 (6.81 million). Roughly 75% of this reduction can be directly attributed to the prior authorization program in the three states listed above. Note: the reduction in approved dialysis transports in New Jersey accounts for nearly half of the national decline). However, that leaves nearly 250,000 fewer approved transports in the remaining 47 states. This reduction was not the result of fewer claims being submitted in 2015; the number of submitted claims was actually higher in 2015 than 2014. Rather, the data shows that this reduction is the result of the MACs actively denying many more claims than in year’s past.
I believe these reductions are the direct result of a step-up in the enforcement activities of the MACs, which I also believe has the tacit, if not outright, approval of CMS.
To test this thesis, I looked at the state-by-state data to see if any trends could be found. What I found was that 28 states saw increases in the total number of approved BLS non-emergency transports in 2015, with 19 states seeing decreases. However, on its face, that number is somewhat deceiving. The states that saw increases tended: (1) to see either relatively small increases or (2) had relatively low utilization rates to begin with. The states that saw decreases tended to be larger states with higher utilization rates, and those decreases tended to be larger in percentage terms. For instance, California saw a 21.5% decrease in the number of approved BLS non-emergency transports. Ohio saw an 11.7% decrease.
Digging deeper, it becomes clear that a state’s overall change in payments for BLS non-emergencies is almost perfectly correlated with its change in payments for dialysis transports. In other words, to the extent the state saw an overall reduction in payments for BLS non-emergencies, that reduction – – in nearly all cases – – was the result of the total payments for dialysis decreasing by more than any offsetting increase in the total payments for non-dialysis transports.
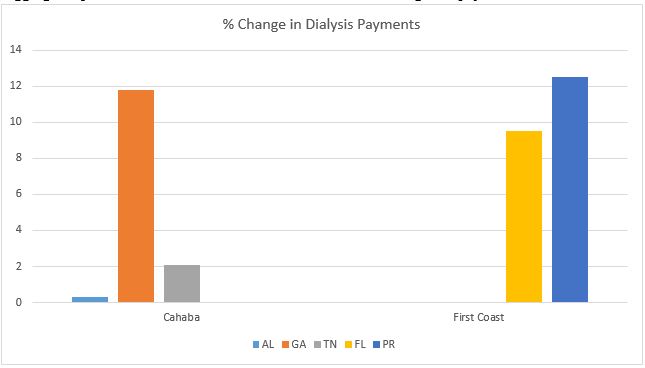
These relative changes in dialysis were also highly correlated with the MAC that administers Medicare claims in that state. To the extent your state saw a reduction in dialysis payments, it is highly likely that neighboring states administered by the same MAC saw similar reductions in payments. The following charts will help illustrate this point:
As you can see, all three states within Cahaba’s jurisdiction saw a net increase in the total payments for dialysis. While the increases themselves were quite minor in Alabama and Tennessee, Georgia saw an 11.8% increase in total payments for dialysis. Similarly, both Florida and Puerto Rico saw significant increases in the approved payments for dialysis.
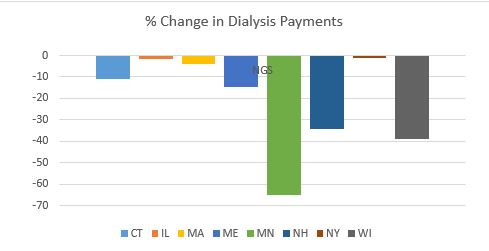
By contrast, every state in National Government Services’ (NGS’) jurisdiction with more than 1,000 paid dialysis transports in 2015 saw a net reduction in the total payments for dialysis. These reductions ranged from a relatively minor reduction of 1.17% in New York to a nearly two-thirds (64.58%) reduction in Minnesota.
This trend was present in all remaining jurisdictions, although the results were more mixed. For example, with the exception of South Carolina, the three remaining states administered by Palmetto all saw increases. Likewise, the majority of states administered by WPS saw decreases. This included Indiana, which has a sizeable dialysis population. Among WPS states, only Missouri saw a small (3.90%) increase.
California saw a 31.76% decrease in its payments for dialysis. The only other Noridian states with more than 1,000 paid dialysis trips were Hawaii and Washington, which both saw increases.
Novitas presents a more complicated picture, with several large states, such as Texas, seeing double-digit increases in payments for dialysis, while other large states saw sizeable decreases.
All in all, the data suggests that CMS and its contractors continue to pay close attention to the non-emergency side of our business, particularly BLS non-emergency transports. These transports have been under scrutiny for many years, as reports from the Office of Inspector General, the Government Accountability Office and other federal agencies have flagged this portion of our industry as being particularly prone to overutilization (and, in some cases, outright fraud). However, this heightened scrutiny is not being uniformly applied across-the-board. The data suggests that certain MACs have been far more aggressive in targeting these sorts of trips across their entire jurisdictions, while others seem content to target specific (typically large) states within their jurisdictions. This could serve as a template for how MACs will approach prior authorization in their jurisdictions.
‘Praemonitus, Praemunitus’
Latin Proverb, loosely translated to “forewarned is forearmed.”



 In honor of today’s
In honor of today’s