HHS Revises Provider Relief Fund Reporting Requirements
This content is for AAA members only.
Please either or Join!
Please either or Join!

Yesterday, Senators Catherine Cortez Masto (D-NV) and Susan Collins (R-ME) introduced the Protecting Access to Ground Ambulance Medical Services Act of 2021 (S. 2037). Senators Cortez Masto and Collins were joined by Senators Debbie Stabenow (D-MI), Bill Cassidy (R-LA), Patrick Leahy (D-VT) and Bernie Sanders (D-VT) as primary cosponsors and leads on the legislation.
S. 2037 is identical to H.R. 2454 by Representatives Terri Sewell (D-AL), Devin Nunes (R-CA), Peter Welch (D-VT) and Markwayne Mullin (R-OK) and would extend the temporary Medicare ground ambulance increases of 2% urban, 3% rural and the super rural bonus payment for five years. The increases are currently scheduled to expire on December 31, 2022. The five-year extension would allow for the increases to remain in place during the two-year delay on ambulance data collection due to the COVID-19 public health emergency, an analysis of the data by MedPAC and subsequent action by the Congress to reform the Medicare ambulance fee schedule.
The legislation would also help ensure that rural zip codes in large urban counties remain rural following geographical changes under the fee schedule as a result of the 2020 census data. The current definition using rural urban commuting areas (RUCA) in Goldsmith Modification areas would be modified for zip codes with 1,000 people or less per square mile would also be rural. Ground ambulance service providers and suppliers could also petition the Centers for Medicare and Medicaid Services (CMS) to make the argument that a specific zip code should be rural. It is vital that this provision be implemented before CMS makes changes from the 2020 census data which will likely occur in 2023.
The AAA has been leading the effort on the legislation with the support of the International Association of Fire Chiefs, International Association of Fire Fighters, National Association of EMTs, National Rural Health Association and the National Volunteer Fire Council.
The AAA will be launching a Call to Action shortly requesting AAA members to ask their Senators to cosponsor S. 2037, and reach out to their Representatives to cosponsor H.R. 2454 if they have not already done so.
We greatly appreciate the leadership of Senators Cortez Masto, Collins, Stabenow, Cassidy, Leahy, and Sanders on this vitally important legislation.
Thank you @SenCortezMasto, @SenatorCollins, @SenBillCassidy, @SenStabenow, @SenatorLeahy, and @SenSanders for collaborating to support America's #EMS providers in the pandemic and beyond! #SupportEMS #AlwaysOpen #MobileHealthcare #NotJustaRide pic.twitter.com/q7Divtby8z
— AmericanAmbulanceAsc (@amerambassoc) June 10, 2021

From CNN on May 22, 2021
America’s rural ambulance services, often sustained by volunteers, are fighting for their survival — a crisis hastened by the impact of Covid-19.
More than one-third of all rural EMS are in danger of closing, according to Alan Morgan, CEO of the National Rural Health Association. “The pandemic has further stretched the resources of our nation’s rural EMS.”

Please either or Join!

Please either or Join!

Please either or Join!
by Kathy Lester, J.D., M.P.H.
As the American Ambulance Association (AAA) reported yesterday, President Trump issued an Executive Order (EO) “An America-First Healthcare Plan.” The EO includes several provisions, including related to drug importation generally and for insulin specifically. It also includes statements that indicate if the Congress does not act before the end of the year, the President will have the Department of Health and Human Services (HHS) “take administrative action to prevent a patient from receiving a bill for out-of-pocket expenses that the patient could not have reasonably foreseen.” It does not mention ground ambulances.
In addition to suggesting action if the Congress does not pass legislation, the EO also states that within 180 days, the Secretary will update the Medicare.gov Hospital Compare website to inform beneficiaries of hospital billing quality, including:
The narrative related to balance billing (surprise coverage) reads as follows:
My Administration is transforming the black-box hospital and insurance pricing systems to be transparent about price and quality. Regardless of health-insurance coverage, two‑thirds of adults in America still worry about the threat of unexpected medical bills. This fear is the result of a system under which individuals and employers are unable to see how insurance companies, pharmacy benefit managers, insurance brokers, and providers are or will be paid. One major culprit is the practice of “surprise billing,” in which a patient receives unexpected bills at highly inflated prices from providers who are not part of the patient’s insurance network, even if the patient was treated at a hospital that was part of the patient’s network. Patients can receive these bills despite having no opportunity to select around an out-of-network provider in advance.
On May 9, 2019, I announced four principles to guide congressional efforts to prohibit exorbitant bills resulting from patients’ accidentally or unknowingly receiving services from out-of-network physicians. Unfortunately, the Congress has failed to act, and patients remain vulnerable to surprise billing.
In the absence of congressional action, my Administration has already taken strong and decisive action to make healthcare prices more transparent. On June 24, 2019, I signed Executive Order 13877 (Improving Price and Quality Transparency in American Healthcare to Put Patients First), directing certain agencies — for the first time ever — to make sure patients have access to meaningful price and quality information prior to the delivery of care. Beginning January 1, 2021, hospitals will be required to publish their real price for every service, and publicly display in a consumer-friendly, easy-to-understand format the prices of at least 300 different common services that are able to be shopped for in advance.
We have also taken some concrete steps to eliminate surprise out‑of-network bills. For example, on April 10, 2020, my Administration required providers to certify, as a condition of receiving supplemental COVID-19 funding, that they would not seek to collect out-of-pocket expenses from a patient for treatment related to COVID-19 in an amount greater than what the patient would have otherwise been required to pay for care by an in-network provider. These initiatives have made important progress, although additional efforts are necessary.
Not all hospitals allow for surprise bills. But many do. Unfortunately, surprise billing has become sufficiently pervasive that the fear of receiving a surprise bill may dissuade patients from seeking appropriate care. And research suggests a correlation between hospitals that frequently allow surprise billing and increases in hospital admissions and imaging procedures, putting patients at risk of receiving unnecessary services, which can lead to physical harm and threatens the long-term financial sustainability of Medicare.
Efforts to limit surprise billing and increase the number of providers participating in the same insurance network as the hospital in which they work would correspondingly streamline the ability of patients to receive care and reduce time spent on billing disputes.
The AAA will continue to advocate for the resources necessary to sustain life-saving mobile healthcare.

The Department of Health and Human Services (HHS) recently announced that it would be extending the deadline for health care providers to apply to receive general distribution funding from the HHS Provider Relief Fund. The deadline to apply for these funds was previously June 3, 2020.
Relevant Background
On March 27, 2020, President Trump signed into law the Coronavirus Aid, Relief, and Economic Security Act (CARES Act). As part of that Act, Congress allocated $100 billion to the creation of a “CARES Act Provider Relief Fund,” which will be used to support hospitals and other healthcare providers on the front lines of the nation’s coronavirus response. An additional $75 billion was allocated as part of the Paycheck Protection Program and Health Care Enhancement Act, bringing the total “Provider Relief Fund” up to $175 billion. This $175 billion will be distributed to health care providers and suppliers to fund healthcare-related expenses or to offset lost revenue attributable to COVID-10.
HHS ultimately elected to allocate these funds through a $50 billion “general allocation,” and multiple smaller “targeted allocations.”
Under its general allocation program, HHS intended to provide health care providers with funds roughly equal to 2% of the provider’s 2018 “net patient revenue,” i.e., the provider’s total revenues from patient care minus provisions for bad debt, contractual write-offs, and certain other adjustments. This general allocation was made in two tranches, with the first tranche being distributed to all providers in mid-April. This first tranche was made based on provider’s 2019 Medicare revenues. As a result, any provider that received payments from the Medicare Fee-for-Service Program in 2019 automatically received an initial relief payment. However, HHS required providers to submit an application to receive relief funding as part of the second tranche. The deadline for applying for the second tranche of relief funding was June 3, 2020.
Scope of New Extension
HHS indicated that the new extension is limited to health care providers that missed the June 3, 2020 deadline to apply for the second tranche of relief funding. The extension also applies to providers that were ineligible for the first tranche of relief funding due to a recent change of ownership. The specific situations that HHS indicated would meet the requirements for the extension include:
Health care providers that meet one of the requirements listed above will have until August 28, 2020 to submit an application for additional relief funds. This deadline aligns with the extended deadline for other eligible Phase 2 providers, such as Medicaid, Medicaid Managed Care, CHIP, and dental providers.
Applications should be submitted through the CARES Provider Relief Fund webpage, which can be found at: https://cares.linkhealth.com/#/.

On July 7, 2020, the Internal Revenue Service published a series of Frequently Asked Questions that address the taxation of payments to health care providers under the HHS Provider Relief Fund.
As part of the Coronavirus Aid, Relief and Economic Security Act (CARES Act), Congress appropriated $100 billion to reimburse eligible health care providers for health care-related expenses and/or lost revenue attributable to the COVID-19 pandemic. The Paycheck Protection Program and Health Care Enhancement Act appropriated an additional $75 billion to the Provider Relief Fund.
The first FAQ addressed the issue of taxation for for-profit health care providers. Specifically, the IRS was asked whether a for-profit health care provider is required to include HHS Provider Relief Fund payments in its calculation of “gross income” under Section 61 of the Internal Revenue Code (Code), or whether such payments were excluded from gross income as “qualified disaster relief payments” under Section 139 of the Code.
The IRS indicated that payment from the Provider Relief Fund do not qualify as qualified disaster relief payments under Section 139 of the Code. As a result, these payments are includible in the gross income of the entity. The IRS further indicated that this holds true even for businesses organized as sole proprietorships.
The second FAQ addressed the issue of taxation for tax-exempt organizations. The IRS indicated that health care providers that are exempt from federal income taxation under Section 501(a) would normally not be subject to tax on payments from the Provider Relief Fund. Notwithstanding this general rule, the IRS indicated that the payment may be subject to tax under Section 511 of the Code to the extent the payment is used to reimburse the provider for expenses or lost revenue attributable to an unrelated trade or business as defined in Section 513 of the Code.
The IRS FAQ can be viewed in its entirety by clicking here. Members are advised to discuss the issue of potential taxation of any relief funding they received with their tax professionals.


July 22, 2020 | 14:00 ET | Register Now for a Reminder!
Join AAA advocacy experts for a fast-paced informal dialogue on Facebook Live! Learn first-hand about EMS advocacy initiatives in the face of COVID-19.
Register to receive a reminder email one hour in advance of the live broadcast on the American Ambulance Association Facebook page!
CMS has issued a blanket waiver modifying the data collection period for the ground ambulance services that were selected to report in Year 1. Under the current law, these organizations would have been required to collect data beginning January 1, 2020, and through December 31, 2020. The waiver allows these organizations to select a new continuous 12-month data collection period that begins between January 1, 2021 and ends December 31, 2021. This modification means that such organizations will collect and report data during the same time period as the ground organizations that CMS will select for Year 2 of the cost collection program.
From the summary of the waiver, it appears that organizations will have the choice of submitting data in Year 1 or Year 2. CMS has not moved the timeline for any other data collection year, so there is the potential for a substantial number of organizations to report in Year 2, which would increase the amount of data available.
The AAA has supported the data collection system to make sure that CMS and the Congress have valid and reliable data to support maintaining the geographic add-ons to the Medicare Ambulance Fee Schedule and to support efforts to address the chronic underfunding of the Medicare Ambulance Fee Schedule.
The complete FAQ is below and also available at: https://www.cms.gov/files/document/summary-covid-19-emergency-declaration-waivers.pdf (on page 29).
“CMS is modifying the data collection period and data reporting period, as defined at 42 CFR § 414.626(a), for ground ambulance organizations (as defined at 42 CFR § 414.605) that were selected by CMS under 42 CFR § 414.626(c) to collect data beginning between January 1, 2020 and December 31, 2020 (year 1) for purposes of complying with the data reporting requirements described at 42 CFR § 414.626. Under this modification, these ground ambulance organizations can select a new continuous 12-month data collection period that begins between January 1, 2021 and December 31, 2021, collect data necessary to complete the Medicare Ground Ambulance Data Collection Instrument during their selected data collection period, and submit a completed Medicare Ground Ambulance Data Collection Instrument during the data reporting period that corresponds to their selected data collection period. CMS is modifying this data collection and reporting period to increase flexibilities for ground ambulance organizations that would otherwise be required to collect data in 2020- 2021 so that they can focus on their operations and patient care.”
“As a result of this modification, ground ambulance organizations selected for year 1 data collection and reporting will collect and report data during the same period of time that will apply to ground ambulance organizations selected by CMS under 42 CFR § 414.626(c) to collect data beginning between January 1, 2021 and December 31, 2021 (year 2) for purposes of complying with the data reporting requirements described at 42 CFR § 414.626.”

On March 27, 2020, President Trump signed into law the Coronavirus Aid, Relief, and Economic Security Act (CARES Act). As part of that Act, Congress allocated $100 billion to the creation of a “CARES Act Provider Relief Fund,” which will be used to support hospitals and other healthcare providers on the front lines of the nation’s coronavirus response. These funds will be used to fund healthcare-related expenses or to offset lost revenue attributable to COVID-10. These funds will also be used to ensure that uninsured Americans have access to testing a treatment for COVID-19. Collectively, this funding is referred to as the “CARES Act Provider Relief Fund.”
On April 9, 2020, the Department of Health and Human Services (HHS) indicated that it would be disbursing the first $30 billion of relief funding to eligible providers and suppliers starting on April 10, 2020. This money will be disbursed via direct deposit into eligible providers and supplier bank accounts. Please note that these are outright payments, i.e., these are not loans that will need to be repaid.
HHS indicated that any healthcare provider or supplier that received Medicare Fee-For-Service reimbursements in 2019 will be eligible for the initial allocation. Payments to practices that are part of larger medical groups will be sent to the group’s central billing office (based on Medicare enrollment information). HHS indicated that billing organizations will be identified by their Taxpayer Identification Numbers (TINs).
Yes. As a condition to receiving relief funding, a healthcare provider or supplier must agree not to seek to collection out-of-pocket payments from COVID-19 patients that are greater than what the patient would have otherwise been required to pay if the care had been provided by an in-network provider.
HHS indicated that the amounts healthcare providers and suppliers will receive will be based on their pro-rata share of total Medicare FFS expenditures in 2019. HHS indicated that Medicare FFS payments totaled $484 billion in 2019.
Providers and suppliers can estimate their initial relief payment amount by dividing their 2019 Medicare FFS reimbursement by $484 billion, and then multiplying that “ratio” by $30 billion. Note: payments from Medicare Advantage plans are not included in the calculation of a provider’s/supplier’s total 2019 Medicare payments.
As an example, HHS cited a community hospital that received $121 million in Medicare payments in 2019. HHS indicated that this hospital’s ratio would be 0.00025. That amount is then multiplied by $30 billion to come up with its initial relief fund payment of $7.5 million.
The AAA has created a CARES Act Provider Relief Calculator
that you can use to estimate your initial relief payment. |
USE DOWNLOADABLE EXCEL CALCULATOR►
No. You do not need to do anything to receive your relief funding. HHS has partnered with UnitedHealth Group (UHG) to disburse these monies using the Automated Clearing House (ACH) system. Payments will be made automatically to the ACH account information on file with UHG or CMS.
Providers and suppliers that are normally paid by CMS through paper checks will receive a check from CMS within the next few weeks.
The ACH deposit will come to you via Optum Bank. The payment description will read “HHSPayment.”
Yes. You will need to sign an attestation statement confirming relief of the funds within 30 days. These attestations will be made through a webportal that HHS anticipates opening the week of April 13, 2020. The portal will need to be accessed through the CARES Act Provider Relief Fund webpage, which can be accessed by clicking here.
You will also be required to accept the Terms and Conditions within 30 days. Providers and suppliers that do not wish to accept these terms and conditions are required to notify HHS within 30 days, and then remit full repayment of the relief funds. The Terms and Conditions can be reviewed by clicking here.
HHS has indicated that it intends to use the remaining relief funds to make targeted distributions to providers in areas particularly impacted by the COVID-19 outbreak, rural providers, providers of services with lower shares of Medicare reimbursement or who predominantly serve Medicaid populations, and providers requesting reimbursement for the treatment of uninsured Americans.

None of the proposals offered so far on an economic stimulus package to address the impact of COVID-19 include our specific provisions to provide ambulance relief! Negotiators on a final package failed to reach an agreement over the weekend. There is still time to influence the final outcome! Please write to your members of Congress!
There are provisions in the packages that would help businesses, first responders and Medicare providers and suppliers. However, the AAA is advocating for specific help for ambulance services with the prioritization of COVID-19 resources, coverage of services, as well as direct financial assistance. The Congress has heard directly from the AAA about our requests and they need to hear from their constituents about assistance to your operations. If you have not yet contacted your members of Congress, please do so today!
Please e-mail today the health aides for your members of Congress!
It will take you only a few minutes per congressional office to email a letter. Just follow these steps.
1. USE LETTER TEMPLATE: CLICK HERE to access a draft letter. Please customize your letter including the cities and towns you serve, if you are sending to the office of a Senator or Representative and any additional details as to services you are providing during the COVID-19 outbreak and the financial impact on your operation.
2. LOOK UP HEALTH STAFFER AND EMAIL ADDRESS: CLICK HERE to access a list of the name of the health staffer and email address for all congressional offices.
3. SEND E-MAILS TO STAFFERS: Copy and paste the email address of the health staffer and copy and paste the letter as the body of the e-mail and send.
While the Congress may not include all of our requests in this stimulus package, there are likely to be future legislative vehicles in which the AAA will continue to press for passage of additional relief for ambulance service organizations and personnel.

The American Ambulance Association has been working hard to accomplish the legislative goals of the membership in the 116th Congress. The AAA would like to take this opportunity to provide an update on what we have accomplished thus far in the 116th Congress.
Balance/surprise billing is a hot button issue that recently came into the spotlight at the start of the 116th Congress. With the President’s announcement calling for Congress to pass legislation that would end surprise billing for patients, there has been an increase in Congressional action on the issue including introduced legislation, discussion drafts and hearings in all committees of jurisdiction. The AAA has been working tirelessly with the Congressional committees of jurisdiction to educate Members and staff on the unique characteristics of EMS systems and that it would be inappropriate to apply the same restrictions on balanced billing to ground ambulance services.
The AAA has formed a working group comprised of AAA member volunteers that have worked on policy and messaging on balance billing. The working group has submitted comments to the Energy and Commerce Committee and Senate HELP committees advocating that the ambulance industry is unique from other stakeholders, and as such, should be looked at differently. Ambulance service providers and suppliers are required by law to treat and transport all patients, regardless of their ability to pay and are heavily regulated at the local level. The AAA has been working to communicate these factors that place the ambulance industry in a different situation than many other stakeholders.
The Public Safety Officers Death Benefit (PSOB), a one-time benefit paid to families of first responders killed in the line of duty, is an issue that the AAA has passionately advocated for over many years. In the 116th Congress, the AAA has secured introduction of legislation in the House of Representatives, H.R. 2887, the Emergency Medical Service Providers Protection Act. H.R. 2887 would extend the PSOB to first responders employed by private for-profit EMS agencies. The AAA was able to secure several commitments from Members of Congress to cosponsor the legislation during Stars of Life meetings in Washington, DC. In addition to taking action to move H.R. 2887 through the legislative process, the AAA will be engaging in an outreach campaign in the next few weeks.
The AAA has worked toward reintroduction of legislation to restructure the offset that was passed into law in the Bipartisan Budget Act of 2018 (H.R. 1892) in the 115th Congress. This offset included a total cut of 23% to the Medicare reimbursement for basic life support (BLS) non-emergency transports performed by all ambulance service suppliers and providers to and from dialysis centers. This cut served as an offset to the 5-year extension of Medicare add on payments that our industry worked hard to get extended.
The AAA has secured introduction of legislation in both the House and Senate. H.R. 3021 was introduced by Representatives LaHood (R-IL) and Sewell (D-AL) and S. 228 by Senators Cassidy (R-LA) and Jones (D-AL). If passed, this legislation would change the cut that is currently in place so that it applies specifically to companies conducting over 50% ESRD non-emergency transports. Those ambulance services with over 50% ESRD transports would get a cut of 29.5%, while those doing less would receive a 15.5% cut. The AAA will continue to work toward movement and passage of this legislation that would better distribute the reduction to those providers which do almost exclusively non-emergency dialysis transports and thus have a lower cost of providing services.
The AAA has crafted legislation that is specifically aimed at addressing major Medicare ambulance industry issues. The issues that will be included in future legislation include making Medicare ambulance add-ons permanent, implementing a prior-authorization program across the nation, allowing for transportation to alternative destinations, reducing regulatory burdens, and providing relief through maintaining many zip codes as rural following the next census. The AAA is working to get this Medicare priorities legislation introduced in the coming months so that we can get to work on solving these Medicare issues that impact our industry as a whole.
Another priority that that the AAA has been diligently working toward getting introduced is Veterans Affairs (VA) legislation. The Veterans Reimbursement for Emergency Ambulance Services Act (VREASA) introduced by Congressman Tipton (R-CO) would provide veterans with reimbursement for emergency ambulance services when a Prudent Layperson would have a reasonable expectation that a delay in seeking immediate medical attention will jeopardize the life or health of the veteran. This legislation was introduced as a result of the VA consistently requiring all medical records be provided, including the records of treatment after the emergency service has taken place. Should those records show that it was not a life threatening emergency or a false alarm, the claim for reimbursement is being denied. The VA legislation would mandate that the VA apply the “prudent layperson” definition of emergency to determine coverage of ambulance claims.
The AAA is also working toward addressing two other issues with the VA to enforce more prompt payment by the VA and treating the VA as the first payor, similar to Medicare, as it is determined whether there is a different primary payor. The AAA has been working with Senators Collins and Tester on language help solve this ongoing and serious reimbursement issue.
In our next update, we will be reporting on the progress the AAA has made this year on regulatory issues.
If you have questions about the discussion draft or balance billing initiatives being undertaken by the AAA, please do not hesitate to contact a member of the AAA Government Affairs Team.
Tristan North – Senior Vice President of Government Affairs
tnorth@ambulance.org | (202) 802-9025
Ruth Hazdovac – AAA Senior Manager of Federal Government Affairs
rhazdovac@ambulance.org | (202) 802-9027
Aidan Camas – Manager of State & Federal Government Affairs
acamas@ambulance.org | (202) 802-9026
Thank you for your continued membership and support
This morning Ruth Hazdovac and Aidan Camas of AAA staff and Kathy Lester, Esq, Healthcare Consultant to the AAA attended a briefing held by the House Energy & Commerce Committee on the issue of surprise/balance billing. At the briefing, staff for Chairman Frank Pallone (D-NJ) and Ranking Member Greg Walden (R-OR) announced that they would be releasing a bipartisan discussion draft, the No Surprises Act, which would “protect consumers from surprise medical bills and increase transparency in our health care system.”
As of now, ground and air ambulances are NOT included in the discussion draft. However, the committee is asking for comments on ground and air ambulance and recommendations on how to provide relief to the consumer in this area. The AAA has a Balance Billing Work Group that is hard at work developing a policy recommendation that will work for our members.
The House Ways and Means Health Subcommittee Chairman Lloyd Doggett also announced today that the Health Subcommittee will hold a hearing next week entitled “Hearing on Protecting Patients from Surprise Medical Bills.” AAA Staff will be at the briefing and provide a timely update to membership on any developments.
The AAA team will be submitting comments and policy recommendations based off the work of the Balance Billing Work Group to both the Energy & Commerce and Ways & Means Committee to ensure that the views of our members are well represented. We will also be reaching out to AAA members in the states of key policymakers on the Committees to submit comments, as well. The AAA will also provide members with key talking points in the event they are contact by their Members of Congress or their staff.
If you have questions about the discussion draft or balance billing initiatives being undertaken by the AAA, please do not hesitate to contact a member of the AAA Government Affairs Team.
Tristan North – Senior Vice President of Government Affairs
tnorth@ambulance.org | (202) 802-9025
Ruth Hazdovac – AAA Senior Manager of Federal Government Affairs
rhazdovac@ambulance.org | (202) 802-9027
Aidan Camas – Manager of State & Federal Government Affairs
acamas@ambulance.org | (202) 802-9026
Thank you for your continued membership and support.

Happy National Rural Health Day! Thank you to all of the ambulance service providers who work hard providing life-saving treatment in rural areas every day.
In part of our ongoing advocacy efforts, the AAA sent a letter today to the Rural Caucuses in the United States Senate and House of Representatives. Addressed to leadership of the caucuses, Sen. Pat Roberts (R-KS), Sen. Heidi Heitkamp (D-ND), Rep. Adrian Smith (R-NE), and Rep. Tim Walz (D-MN), this in-depth letter highlights the critical work that our members do every day around the country and raises important issues affecting the industry. Issues covered in the letter include:
The letter also highlights some of the burdensome regulations facing ambulance service providers that the AAA has recommended Congress address through its Red Tape initiative. These include:
This letter from the AAA to Congressional leaders is just one part of the AAA’s ongoing effort to educate Congress on the crucial role ambulance service providers play in America’s healthcare system. The AAA wants Congress to know that in many rural areas of the country, ambulances are the medical safety net, yet face extreme challenges to staying in business thanks to below cost reimbursement and burdensome regulations. The AAA will continue to pursue this list of priorities with our members next year and going forward.
Again, Happy Rural Health Day to our members – thanks for all that you do!
If you have any questions about our letter or rural advocacy, please contact us:
If you have questions about the legislation or regulatory initiatives being undertaken by the AAA, please do not hesitate to contact a member of the AAA Government Affairs Team.
Tristan North – Senior Vice President of Government Affairs
tnorth@ambulance.org | (202) 802-9025
Ruth Hazdovac – AAA Senior Manager of Federal Government Affairs
rhazdovac@ambulance.org | (202) 802-9027
Aidan Camas – Manager of State & Federal Government Affairs
acamas@ambulance.org | (202) 802-9026
Thank you for your continued membership and support.
On October 1, 2018, CMS implemented an additional thirteen (13%) cut in reimbursement for non-emergency BLS transports to and from dialysis. This cut in reimbursement was mandated by Section 53108 of the Bipartisan Budget Act of 2018. This on top of a ten (10%) cut in reimbursement for dialysis transports that went into effect on October 1, 2013. As a result, BLS non-emergency ambulance transports to and from dialysis that occur on or after October 1, 2018 will be reimbursed at 77% of the applicable Medicare allowable.
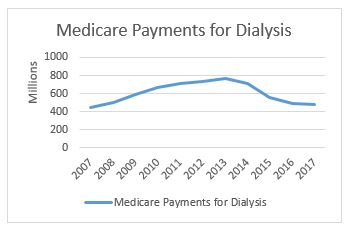
In related news, CMS has released its national payment data for calendar year 2017. This data shows a continued reduction in total Medicare payments for dialysis transports. Medicare paid $477.7 million on dialysis transports in 2017, down from $488.9 million in 2016. This continues a downward trend that has seen total payments decline from a high of more than $750 million in 2013 (see accompanying chart to the right). Not coincidentally, it was in 2013 that our industry saw its first reduction in Medicare’s payments for dialysis transports.
The payment reduction is partially the result of the reduction in the amounts paid for dialysis services. However, it is also reflective of an overall decline in the number of approved dialysis transports. For this, we can look primarily to the impact of a four-year demonstration project that requires prior authorization of dialysis transports in 8 states and the District of Columbia.
As a reminder, the original prior authorization states were selected based on higher-than-average utilization rates and high rates of improper payment for these services. In particular, the Medicare Payment Advisory Commission (MedPAC) had singled out these states as having higher-than-average utilization of dialysis transports in a June 2013 report to Congress. The chart below shows total spending on dialysis in those states in the years immediately preceding the implementation of the prior authorization project up through 2017, the third year of the demonstration project. While the three states had very different trajectories prior to 2015, each showed a significant decrease in total payments for dialysis under the demonstration project.
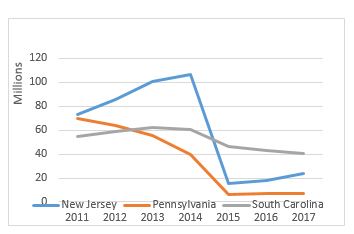
However, it is the trajectory of these changes that I want to discuss in this month’s blog. In previous blogs, I discussed the impact of the particular Medicare Administrative Contractor on the outcomes under prior authorization. Specifically, I noted that, while dialysis payments dropped in each state, the decline was far more dramatic in the states administered by Novitas Solutions (NJ, PA) than in the South Carolina, which was administered by Palmetto GBA. This trend continued in the second year of the program, which saw prior authorization expanded into five additional states and the District of Columbia. Those states administered by Novitas (DE, MD) saw far greater declines than the states administered by Palmetto (NC, VA, WV).
Given these declines, the data from the third year is somewhat surprising. The states administered by Palmetto continued to see declines in total dialysis payments, with the only exception being West Virginia. However, in the states administered by Novitas, we saw total dialysis payments increase, particularly in New Jersey, which saw nearly a 33% increase in total dialysis payments.
Three years into the prior authorization program, it is starting to become clear that the two MACs have approached the problem of overutilization of dialysis transports using two different approaches. Palmetto appears to have adopted a slow-and-steady approach, with total payments declining in a consistent manner year after year. By contrast, Novitas adopted more of a “shock the system” approach, where it rejected nearly all dialysis transports in the first year, and has adopted a somewhat more lenient approach in subsequent years.
Last year, I wrote that two years of data under the prior authorization program permitted two conclusions: (1) the implementation of a prior authorization process in a state will undoubtedly result in an overall decrease in the total payments for dialysis within that state and (2) the size of that reduction appears to be highly dependent on the Medicare contractor.
With an additional year of data, I think both conclusions remain valid, although I would revise the second to suggest that the initial reduction has more to do with the Medicare contractor. The evidence from the third year of the program suggests that the trends tend to equalize after the first few years. It is also possible that Novitas felt a more aggressive approach was needed in the first few years to address evidence of widespread dialysis overutilization in the Philadelphia metropolitan area.
This has potential implications beyond the demonstration project, as CMS looks towards a possible national expansion of the program. Among other issues, it suggests that the AAA must continue its efforts to work with CMS and its contractors on developing more uniform standards for coverage of this patient population.
The AAA continues to work on legislation that would restructure this cut to dialysis transport reimbursement. The AAA strongly supports the NEATSA Act (H.R.6269) introduced by Congressman LaHood (R-IL) and Congresswoman Sewell (D-AL) that would restructure the offset so that a majority of the additional reduction would be focused on those ambulance service agencies in which 50% or more of their volume are repetitive BLS nonemergency transports. AAA members and the AAA are working to get a Senate companion bill introduced shortly. The goal of this legislation would be to have the restructured offset go into effect as soon as possible. Thank you to the dozens of AAA members who have already contacted their members of Congress voicing their support for this critical legislation.
Have an issue you would like to see discussed in a future Talking Medicare blog? Please write to me at bwerfel@aol.com
The AAA continues to press policy initiatives with Congress and the Administration that are important to our members. While not as high-profile as our successful efforts earlier this year on the five-year extension of the Medicare ambulance add-ons, the AAA is working hard on ambulance legislation and regulations that impact the EMS industry and ambulance services across the country. Here is a snapshot of those current efforts. Over the next month, we will be providing weekly in-depth updates highlighting these issues.
The AAA was successful in getting our preferred language of an ambulance cost data collection system using a survey and random sample methodology included with the extension of the add-ons in the Bipartisan Budget Act of 2018. However, that was just the first key step in the process. We now need to ensure that CMS gets the details right as the agency develops the structural specifics and data elements for the system. It is critical that the system is designed in a way that ambulance service suppliers and providers will submit the most accurate data possible.
The data will ultimately provide the information necessary for Congress, the Centers for Medicare and Medicaid Services (CMS) as well as the AAA and other stakeholders to reform the Medicare ambulance fee schedule. Reform will include potential reimbursement for services such as community paramedicine, treat and refer, and other items that don’t involve transporting the patient. However, in order to determine the reimbursement levels, we first need the data on what it could cost for these additional services. The AAA therefore has been working closely with officials at CMS on the development of the data collection system.
The five-year extension of the add-ons and authorization of data cost collection system were the first steps needed in the long-term goal of reforming the Medicare ambulance fee schedule. The AAA is now developing the next piece of legislation as step two of the process. The “Community Bill” would make the Medicare ambulance add-ons permanent, treat ambulance service suppliers like providers in three specific instances, direct the Centers for Medicare and Medicaid Services (CMMI) to do additional pilot programs on innovative services being done by ambulance agencies, reduce regulatory burdens, and implement a more accurate definition of what Goldsmith Modification zip codes should remain as rural. The AAA is currently developing the draft bill and reaching out to congressional offices regarding the introduction of the bill which will likely occur early next Congress.
The AAA is supporting the efforts of our members who would be significantly adversely affected by the upcoming reduction in dialysis transport reimbursement to restructure the cut. Congress included in the Bipartisan Budget Act of 2018 an offset to go along with the extension of the add-ons that will cut reimbursement for BLS nonemergency transports to and from dialysis centers by an additional 13%. This will be on top of the existing 10% reduction. The NEATSA Act (H.R.6269) by Congressman LaHood (R-IL) and Congresswoman Sewell (D-AL) would restructure the offset so that a majority of the additional reduction would be focused on those ambulance service agencies in which 50% or more of their volume are repetitive BLS nonemergency transports. The cut is currently scheduled to be implemented on October 1 and impacted AAA members and the AAA are working to get a Senate companion bill introduced shortly.
As an amendment to the Farm Bill (S. 3042) that passed the Senate, Senator Dick Durbin (D-IL) included language similar to the SIREN Act (S. 2830, H.R. 5429) to reauthorize the Rural EMS Grant program. However, in an effort to ensure the funding would go to the most needy, small, and rural EMS providers, the language of the amendment and SIREN Act would change the eligibility to just governmental and non-profit EMS agencies. Therefore, small rural for-profit ambulance service providers would no longer be eligible to apply for grants.
The AAA is pressing Senator Durbin as well as other members supportive of the reauthorization to revise the language to ensure small rural for-profit providers would still be able to apply for grants. In the next few weeks, the AAA will be asking AAA members to reach out to their members of Congress in support of the final Farm Bill including the reauthorization language and that it continues to also apply to for-profit providers as well.
Over the last year, the AAA has responded to several requests for information from CMS as well as Congress on how to ease regulatory burdens for Medicare providers and suppliers. In addition to these broader opportunities, representatives of the AAA and our members have been meeting with CMS officials to reduce burdens for our industry. As a specific example, we are pushing for the elimination of the PCS for interfacility transports and to expand the categories of facility personnel eligible to sign the form.
The AAA continues to educate members of Congress and congressional staff about the importance of non-emergency ambulance services. We are providing congressional offices with a clearer picture as to the vital role of these transports as part of the overall health care system. We are also looking to ensure that changes in federal payor policies strengthen the role and distinction of non-emergency ambulance transports from non-medical transportation services to health care facilities.
The current use of Rural-Urban Commuting Areas (RUCA) as the basis of the Goldsmith Modification for determining rural areas in larger urban counties needs to be reformed. There are numerous examples of zip codes that are designated as urban under the Medicare ambulance fee schedule that are clearly rural. The AAA Rural Task Force is leading the way on both short-term and long-term efforts to more accurately capture rural zip codes in large urban counties. The AAA will include the ultimate reform provision crafted by the Task Force within the Community Bill as well as look at other legislative opportunities to make the changes.
If you have questions about the legislation or regulatory initiatives being undertaken by the AAA, please do not hesitate to contact a member of the AAA Government Affairs Team.
Tristan North – Senior Vice President of Government Affairs
tnorth@ambulance.org | (703) 610-0216
Ruth Hazdovac – AAA Senior Manager of Federal Government Affairs
rhazdovac@ambulance.org | (703) 610-5821
Aidan Camas – Manager of State & Federal Government Affairs
acamas@ambulance.org | (703) 610-9039
Thank you for your continued membership and support.
While the Congress succeeded in passing the Republican tax bill and keeping the federal government open with a short-term continuing resolution that included a temporary extension for the State Children’s Health Insurance Program (CHIP), it did not act upon the several Medicare extenders that expire on December 31, 2017. This extenders package includes the ambulance add-ons for urban, rural, and super-rural areas, as well as a moratorium on therapy caps, extenders for hospitals, and several other extenders important to other Medicare providers.
Despite the fact that the Congress left town, there is still strong bipartisan support for reinstating these extenders – including the ambulance extenders – early in January 2018. The most likely time frame will be for the extenders to be added to the next government funding legislation, which must be passed by January 19.
First, do not panic. As you may have already heard, CMS is telling providers and suppliers that the add-ons will expire at the end of the month. Technically that is true. The Agency is simply stating the obvious; but no one should imply from such statements that the Congress will not fix them or not make them retroactive. Historically, CMS has followed this pattern of indicating the add-ons have expired until legislation extending the add-ons has passed both chambers of Congress and the President has signed the bill into law. CMS will make similar statements relative to the other Medicare extenders as well.
Second, prepare. To the extent you are able to do so, you may hold your claims. Medicare requires providers to files claims no later than 12 months after the date when the services were provided. (See Medicare: File a Claim; see also section 6404 of the Affordable Care Act). While this may not work for all claims, holding claims will reduce the number that would have to be reprocessed once the add-ons become law. If CMS believes at some point the legislation will pass, it may also break with its own precedent and indicate that has asked the contractors to hold claims for a short period of time as well. It did this in 2014 when it discovered errors in a final fee schedule rule. Once the claims are processed, so long as the add-ons have been extended by law, the add-on dollars will appear in the reimbursement amounts sent to providers and suppliers.
Third, retroactivity can be expensive, but CMS can mitigate the costs. CMS did this most recently in May of 2017. Then, CMS announced that it would implement the retroactive extension of a transitional payment for durable medical equipment suppliers by having the contractors automatically reprocess claims from the period when the transitional payment was made retroactive. This approach reduced the burden on providers and suppliers by eliminating the need to resubmit claims.
Despite the fact that there are ways to mitigate the problem, the American Ambulance Association (AAA) remains deeply concerned that the Congress did not extend the add-ons before they left for the holidays. We understand that for ambulance services across the country receiving timely payments from Medicare can be the difference between being able to make payroll or not. Having the dollars from the add-ons is also crucial to ensuring adequate cash flow. Therefore, while we advise you to think through your options and take the steps that best meet your needs and the needs of your employees, patients, partners, and businesses, we also ask that you reach out to the Congress and let them know how important it is to get the add-ons extended as early in January as possible. Make your voice heard by going to the AAA’s grassroots page. There you can send an email or reach out through social media to your Members of Congress. We need everyone, including your employees, patients, and others who support high quality ambulance services, to reach out today.
Write to Your Members of Congress
The AAA will continue our direct efforts on Capitol Hill to make sure these add-ons are extended and overly burdensome new requirements are not placed on ambulance services. With your help, we can get the add-ons extended. For more information please visit https://ambulance.org/advocacy/.

The current 33-month extension of the Medicare add-on payments is set to expire at the end of December 2017. Losing these add-on payments would be a devastating blow to ambulance services across the country. It is crucial that the payments be extended as we push for a long-term solution. H.R. 3236 introduced by Reps. Nunes, Upton, and Welch would extend the current temporary Medicare add-ons for five years. More details about the Bill can be found below. Let your Representative know that you support H.R. 3236 — Here are three quick and easy ways to get involved!
Writing to your members of Congress only takes 2 clicks, follow these simple steps:
1. Enter contact information below (required by Congressional offices) and click “Submit”
2. On the next page you’ll see the letter to your Representative (Message 1) and the letter(s) to your Senators (Message 2) – click “Submit Messages”
Feel free to personalize your letter(s) before submitting them.

Post on Facebook why H.R. 3236 is important! Be sure to tag your Representative and encourage others to share your post! Ask others to write letters of support as well! http://bit.ly/AAAbill
More About Our Bill H.R. 3236, the Ambulance Medicare Budget and Operations Act of 2017:
Legislation to extend the Medicare ambulance add-on payments for five years has been introduced by Representatives Nunes, Upton, and Welch (H.R. 3236).
Specifically, the bill: