
National Ambulance Provider and Supplier Coalition Meeting: May 22, 2025
This content is for AAA members only.
Please either or Join!
Please either or Join!

On August 26, 2021, the Centers for Medicare and Medicaid Services (CMS) announced its proposed timeline for the national expansion of the Prior Authorization Model for Repetitive, Scheduled Non-Emergent Ambulance Transports (RSNAT). The formal notice appeared in the Federal Register on August 27, 2021.
Background
In December 2014, the Centers for Medicare and Medicaid Services (CMS) implemented a prior authorization model for payment of repetitive, scheduled non-emergent ambulance transportation. Under this Model, ambulance suppliers are required to seek and obtain prior authorization for the transportation of repetitive patients beyond the third round-trip in a 30-day period. Absent prior authorization, the Medicare Administrative Contractors (MACs) are required to subject further claims to prepayment review.
The Model was initially implemented in three states: New Jersey, Pennsylvania, and South Carolina. These “Year 1” states were selected based on relatively high per-capita expenditures on RSNAT. The Model was subsequently expanded in January 2016 to five additional states (Delaware, Maryland, North Carolina, Virginia, and West Virginia) and to District of Columbia. These “Year 2” states were selected based on their inclusion in the same MAC Jurisdiction as one or more of the Year 1 states.
The purpose of the RSNAT Model was to test whether prior authorization would be effective in reducing Medicare expenditures on RSNAT, without adversely impacting beneficiary access to medically necessary services. CMS engaged Mathematica, a public health care research firm, to study the impact of prior authorization on ambulance utilization in the demonstration states. Mathematica issued several reports that concluded that the Model was effective in reducing Medicare expenditures without any measurable impact on the quality of care available to Medicare beneficiaries.
On November 23, 2020, CMS published a notice in the Federal Register indicating that it intended to expand the Prior Authorization Model to all remaining states and U.S. territories. However, citing the current Public Health Emergency, CMS elected not to set a timeline for that national expansion.
The current notice announces that timeline for national expansion
Expansion Timeline
CMS has indicated that the RSNAT Model will be expanded into new states on the following timeline:
| Expansion Date | Affected States |
| December 1, 2021 | Arkansas, Colorado, Louisiana, Mississippi, New Mexico, Oklahoma, and Texas |
| Not earlier than
February 1, 2022 |
Alabama, California, Georgia, Hawaii, Nevada, Tennessee, American Samoa, Guam, and the Northern Mariana Islands |
| Not earlier than
April 1, 2022 |
Florida, Illinois, Iowa, Kansas, Minnesota, Missouri, Nebraska, Wisconsin, Puerto Rico, and the U.S. Virgin Islands |
| Not earlier than
June 1, 2022 |
Connecticut, Indiana, Maine, Massachusetts, Michigan, New Hampshire, New York, Rhode Island, and Vermont |
| Not earlier than
August 1, 2022 |
Alaska, Arizona, Idaho, Kentucky, Montana, North Dakota, Ohio, Oregon, South Dakota, Utah, Washington, and Wyoming |
An analysis of the proposed timeline suggests that CMS has elected to expand the RSNAT Model based on existing Medicare Administrative Contractor (MAC) Jurisdictions. For example, each of the states slated to be included in the December 1, 2021 expansion fall within MAC Jurisdiction H. This MAC Jurisdiction is administered by Novitas Solutions, Inc. Novitas also administers MAC Jurisdiction L, which has been operating under the RSNAT Model since 2014. Thus, CMS likely selected MAC Jurisdiction H for the first stage of the national expansion due to Novitas’ experience in administering the RSNAT Model.
The second stage of the national expansion will occur no earlier than February 1, 2022. This stage will include all states and territories located in MAC Jurisdiction J and MAC Jurisdiction E. MAC Jurisdiction J is administered by Palmetto GBA, LLC, which has been administering the RSNAT Model in MAC Jurisdiction M since 2014. MAC Jurisdiction E is administered by Noridian Healthcare Solutions, LLC. This will be Noridian’s first experience with the RSNAT Model.
The third stage of the national expansion will occur no earlier than April 1, 2022. This stage will include all states and territories located in MAC Jurisdiction 5 (Wisconsin Physicians Service Government Health Administrators), MAC Jurisdiction 6 (National Government Services, Inc.), and MAC Jurisdiction N (First Coast Service Options, Inc.)
The fourth stage of the national expansion will occur no earlier than June 1, 2022. This stage will include all states and territories located in MAC Jurisdiction 8 (Wisconsin Physicians Service Government Health Administrators) and MAC Jurisdiction K (National Government Services, Inc.).
The final stage of the will occur no earlier than August 1, 2022. This stage will include all states and territories located in MAC Jurisdiction 15 (CGS Administrators, LLC) and MAC Jurisdiction F (Noridian Healthcare Solutions, LLC).
Outreach and Education
With the formal announcement of CMS’ timeline for the national expansion of the RSNAT Model, the American Ambulance Association will be increasing its educational efforts related to prior authorization. This will include webinars and other educational materials on the technical elements of the prior authorization process, the importance of third-party documentation, as well as basic best practices related to the transportation of repetitive patients. We encourage all members that may be impacted by the expansion of prior authorization to take advantage of these educational materials.

On April 1, 2019, CMS implemented a new series of Common Working File (CWF) edits that it stated would better identify ground ambulance transports that were furnished in connection with an outpatient hospital service that would be bundled to the skilled nursing facility (SNF) under the SNF Consolidated Billing regime.
Unfortunately, the implementation of these new edits has been anything but seamless. Over the past few weeks, I have received numerous phone calls, texts, and emails from AAA members reporting an increase in the number of Medicare claims being denied for SNF Consolidated Billing.
This FAQ will try to explain why you may be seeing these denials. I will also try to provide some practical solutions that can: (1) reduce the number of claims denied by the edits and (2) help you collect from the SNFs, when necessary.
Please note that, at the present time, there is no perfect solution to this issue, i.e., there is nothing that you can do to completely eliminate these claim denials. The solutions discussed herein are intended only to minimize the disruption to your operations caused by these denials.
Under the SNF Consolidated Billing regime, SNFs are paid a per diem, case-mix-adjusted amount that is intended to cover all costs incurred on behalf of their residents. Federal regulations further provide that the SNF’s per diem payment generally the cost of all health care provided during the beneficiary’s Part A stay, whether provided by the SNF directly, or by a third-party. This also includes the majority of medically necessary ambulance transportation provided during that period. For these purposes, the “Part A Period” refers to the first 100 days of a qualified SNF stay.
However, medically necessary ambulance transportation is exempted from SNF Consolidated Billing (referred to hereafter as “SNF PPS”) in certain situations. This includes medically necessary ambulance transportation to and from a Medicare-enrolled dialysis provider (whether free-standing or hospital-based). Also excluded are ambulance transportations:
For a fuller description of the SNF Consolidated Billing Regime, including a discussion of when ambulance services may be separately payable by Medicare Part B, I encourage members to consult the AAA Medicare Reference Manual.
Purchase the 2019 Medicare Reference Manual
In 2017, the HHS Office of the Inspector General conducted an investigation of ground ambulance claims that were furnished to Medicare beneficiaries during the first 100 days of a skilled nursing home (SNF) stay. The OIG’s investigation consisted of a review of all SNF beneficiary days from July 1, 2014 through June 30, 2016 to determine whether the beneficiary day contained a ground ambulance claim line. The OIG excluded beneficiary days where the only ambulance claim line related to: (1) certain emergency or intensive outpatient hospital services or (2) dialysis services, as such ambulance transportation would be excluded from SNF Consolidated Billing.
The OIG determined that there were 58,006 qualifying beneficiary days during this period, corresponding to $25.3 million in Medicare payments to ambulance suppliers. The OIG then selected a random sample of 100 beneficiary days for review. The OIG determined that 78 of these 100 beneficiary days contained an overpayment for the associated ambulance claims, as the services the beneficiary received did not suspend or end their SNF resident status, nor was the transport for dialysis. The OIG determined that ambulance providers were overpaid a total of $41,456 for these ambulance transports. The OIG further determined that beneficiaries (or their secondary insurances) incurred an additional $10,723 in incorrect coinsurance and deductibles. Based on the results of its review, the OIG estimates that Medicare made a total of $19.9 million in Part B overpayments to ambulance suppliers for transports that should have been bundled to the SNFs under SNF Consolidated Billing regime. The OIG estimated that beneficiaries (and their secondary insurances) incurred an additional $5.2 million in coinsurance and deductibles related to these incorrect payments.
The OIG concluded that the existing edits were inadequate to identify ambulance claims for services associated with hospital outpatient services that did not suspend or end the beneficiary’s SNF resident status, and which were not related to dialysis. The OIG recommended that CMS implement additional edits to identify such ambulance claims.
The OIG’s report prompted CMS to issue Transmittal 2176 in November 2018. This transmittal instructed the CWF Maintainer and the Medicare Administrative Contractors (MACs) to implement a new series of edits, effective April 1, 2019.
Before we turn to the new edits, I think it is important to understand that CMS has had long-standing edits to identify outpatient hospital services that should be bundled to the SNF under SNF PPS. These edits work by comparing the Healthcare Common Procedure Coding System (HCPCS) or Current Procedural Terminology (CPT) codes on the outpatient hospital claim to applicable lists of excluded codes. To the extent the HCPCS or CPT code appears on the applicable list of excluded codes, the outpatient hospital claim will bypass the edit for SNF PPS, and be separately payable by the MAC. To the extent the HCPCS or CPT code on the outpatient hospital claim does not appear on the applicable list of excluded codes, the claim will be denied as the responsibility of the SNF. The new CWF edits for ambulance claims simply extend the existing process one step further, i.e., they compare the ambulance claim to the associated hospital claim.
Conceptually, the new edits “staple” the ambulance claim to the outpatient hospital claim, with our coverage piggybacked on whether the outpatient hospital claim is determined to be bundled or unbundled.
Typically, the denial will be evidenced by a Claim Adjustment Reason Code on the Medicare Remittance Advice. The denial will typically appear as an “OA-190” code, with the following additional explanation: “Payment is included in the allowance for a Skilled Nursing Facility (SNF) qualified stay. The “OA” stands for “Other Adjustment,” and is intended to notify you that the SNF is the correct payer. Note: in some instances, the denial may appear as “CO-190” on the remittance advice. However, the effect of the denial is the same, i.e., they are indicating that the SNF is financially responsible for payment.
Frequently, the denial will be accompanied by Remittance Advice Remark Code “N106,” which indicates “Payment for services furnished to Skilled Nursing Facility (SNF) inpatients (except for excluded services) can only be made to the SNF. You must request payment from the SNF rather than the patient for this service.”
When CMS elects to implement a new edit to the CWF, it has to make some decisions on how to structure the edit. Two typical decisions that must be made are:
For these purposes, a conditional edit is one where the coverage or lack of coverage depends, in part, on the claims submitted by other health care providers that furnished services to the same beneficiary (typically on the same date). As you are probably aware, the Medicare rules for all Part B payments prohibit payment whenever the service has been paid for, directly or indirectly, under Medicare Part A. Thus, all edits for hospital and SNF bundling are conditioned, in part, on the patient’s Part A inpatient status at the time of transport.
By contrast, an unconditional edit is one that operates the same regardless of other types of claims for the same patient. For example, with respect to ambulance claims, the MACs medical necessity edits are unconditional, i.e., they apply to all ambulance claims, regardless of the patient’s inpatient status at a Part A facility. The edits for origin/destination modifiers are another example of an edit that is typically unconditional.
In addition, CMS has to decide whether to make an edit under- or over-inclusive. This is because no edit can be perfectly tailored to be applied to all qualifying claims, but no non-qualifying claims. An “underinclusive” edit is one that is designed to identify the majority – – but not all – – of the claims that should be denied based on the edit criteria. By contrast, an “overinclusive” edit is one that would deny not only all of the qualifying claims, but also some non-qualifying claims.
In many instances related to EMS coverage, the underlying facts and circumstances of the transport are ultimately what determines the coverage. It is frequently difficult – – if not impossible – – to fully describe these circumstances with enough specificity on the electronic claim for CMS to perfectly apply its edits. For that reason, CMS has historically elected to design its ambulance edits to be underinclusive.
Unfortunately, the new SNF edits are both conditional AND overinclusive. To further complicate matters, they are not only conditioned on the claim of a single Part A provider, but two separate Part A providers, i.e., in order for the new edits to work properly, CMS is reliant upon information from both the SNF and the hospital to properly apply its new edits.
They are. The denial was likely the result of your claim being submitted prior to Medicare’s receipt of the associated outpatient hospital claim.
As noted above, the new edits are both conditional and overinclusive. In this context, they are designed to deny the ambulance claim UNLESS there is a hospital outpatient claim for that same patient with the same date of service. If there is no hospital outpatient claim on file when your ambulance claim hits the system, the edit indicates that the MAC should deny your claim for SNF PPS.
In theory, no. The instructions in Transmittal 2176 make clear that the CWF should “adjust” the ambulance claim upon receipt of the associated hospital claim. For these purposes, that adjustment should take the form of re-processing the ambulance claim through the edits to compare it to the associated hospital claim, and to bypass the new CWF edits if the hospital claim contains an excluded code.
However, there is no timeframe for how quickly these adjustments should take place. Most ambulance providers are reporting that they are seeing few, if any claims, being reprocessed.
As noted above, the edits were designed to deny claims to the extent CMS was unable to determine whether they should be bundled to the SNF, i.e., to deny if the associated hospital claim was not already in the system. Therefore, in theory, it should be impossible for the ambulance provider to receive a payment and then a recoupment for SNF PPS.
I suspect the situation described above is one where the ambulance claim is submitted prior to CMS’ receipt of the associated SNF claim for the patient. As noted above, in order for the edits to work properly, both the associated hospital and SNF claims must be in the system. While CMS clearly contemplated the possibility that the ambulance claim might be submitted prior to the associated hospital claim, they do not appear to have considered the possibility that the ambulance claim might beat the associated SNF claim into the system.
When that happens, there is nothing in the CWF to indicate that the patient was in a Part A SNF Stay. As a result, the claim bypasses these new edits entirely, and frequently ends up being paid by the MAC. I suspect what happens next is that the SNF claim hits the system, and triggers CMS to automatically recoup the payment for the ambulance claim.
What should happen at that point is the ambulance claim should then be run through the new edits. If the hospital claim is already in the system, the ambulance claim gets “stapled” to that claim, and then either passes the edit or gets denied based on the information on the hospital claim. If the hospital claim is not in the system, the ambulance provider gets the “interim” denial discussed above, and the claim should be further adjusted if and when the hospital claim is submitted.
However, at this point, it is entirely possible that these claims are not being put through the edit. The AAA has asked CMS to look into whether the new edits are working as intended in these situations.
Not really a question, but you are not wrong.
I think it is important to distinguish between: (1) denials that are correct based on the HCPCS or CPT codes on the associated hospital claim and (2) denials that are based solely on the timing of your claim, i.e., denials based on your claim being submitted prior to the submission of the associated hospital claim. For these purposes, I will refer to the latter category as “interim denials.”
At the onset, I think all members should recognize that there is nothing you can do to eliminate denials for claims that are properly bundled to the SNF based on the HCPCS or CPT codes on the associated hospital claim.
For numerous reasons, I think the proper focus should be on reducing the interim denials. First and foremost, the difficulty with an interim denial is that you don’t know whether that denial will ultimately prove to be correct, or whether the claim will ultimately be reprocessed and paid by the MAC. Second, even if the claim will be reprocessed, there currently appears to be a significant delay in “when” that reprocessing takes place. Finally, without knowing whether the claim will be reprocessed (and whether that reprocessing will result in a payment), you can’t know whether you should be billing the SNF.
You would need to know the following data points prior to the submission of your claim:
If you knew with certainty that the patient was not in the Part A Period of their SNF stay, you would know that the new edits would be inapplicable to your claim, and you could submit it to Medicare as part of your normal billing workflow.
If you also knew the specific procedure/service the patient received at the hospital, you would also be in a position to know whether the service was the financial responsibility of the SNF, assuming the patient was in the Part A Period. When you know the claim is the financial responsibility of the SNF, you could then immediately invoice the claim to the SNF. If your arrangement with the SNF requires you to first obtain a Medicare denial, you would also have the option of submitting the claim and getting the proper OA-190 denial, and then invoicing the SNF. Note: in these situations, you would receive the oA-190 denial regardless of whether your claim was submitted prior to the hospital claim.
By contrast, when you know the patient is in the Part A Period AND the procedure/service is one that would be excluded from SNF PPS, you can avoid the interim denial by ensuring that your claim is not submitted until after the associated hospital claim. In other words, this is a situation where holding your claim for a reasonable period of time might be beneficial.
First, they are absolutely permitted to share this information with you. Both you and the SNF are “covered entities” under the HIPAA Privacy Rule. In this instance, information on the patient’s Part A status would be helpful to you in managing your payment practices. The regulations at 45 C.F.R. 164.506(c)(3) permit one covered entity to share protected health information with another covered entity for the payment activities of that entity.
However, it is important to note that, while the SNF may share that information with you, the Privacy Rule does not require them to provide you with this information absent a written authorization from the patient.
This information is critical to navigating the new edits. If you haven’t been asking for it up until this point, I would strongly encourage you to consider having a discussion with the local SNFs to explain why you will be asking for this information in the future. You may also want to consider developing a specific form that they must complete (similar to the PCS form) that would provide this information.
I understand. I would try to explain to the SNF that the reason you are asking for this information is to be able to make an intelligent determination on whether the transport is likely to the be financial responsibility of the SNF. This information allows you to avoid denials in certain instances where they would otherwise not be responsible. If they don’t provide you with this information, the foreseeable consequence is that you will end up getting interim denials from Medicare, which may leave you no choice but to bill the SNF for the transport.
You do. I would try to insert language into your agreements with the SNFs that obligate them to provide you with this information. You could also try to insert language that makes them financially responsible whenever they fail to provide this information.
One of the foreseeable consequences of this new edit is that it will increase the frequency with which you bill the SNFs. One of the most common complaints I hear is that SNFs refuse to pay their bills. In most instances, the problem is that the ambulance service lacks a written agreement with the SNF, and, as a result, they frequently end up in disputes about when the SNF is responsible. A written agreement that clearly spells out when the SNF is responsible can not only minimize the potential for misunderstandings, but also afford you greater remedies when the SNF refuses to pay.
You should consult with your local attorney regarding the applicable language. However, conceptually, you want to include language that indicates that a Medicare denial is conclusive evidence that the SNF is financially responsible. This provision could then go on to provide that, in the event Medicare should reprocess and pay a particular claim, then you would refund the SNF’s payment.
The AAA is currently conducting a survey of members to help get a sense of the magnitude of the issues created by these new edits. If you would like to participate in the survey, you can click here.
Have an issue you would like to see discussed in a future Talking Medicare blog? Please write to me at bwerfel@aol.com.

On April 1, 2019, CMS implemented a new series of Common Working File (CWF) edits that are intended to better identify ground ambulance transports that are furnished in connection with an outpatient hospital service that is properly bundled to the skilled nursing facility (SNF) under the SNF Consolidated Billing regime.
These edits work by comparing the ambulance claim to the associated outpatient hospital claim. Hospital claims were already subject to CWF edits designed to identify outpatient hospital services that should be bundled to the SNF. These hospital edits operate by referencing a list of Healthcare Common Procedure Coding System (HCPCS) or Current Procedural Terminology (CPT) codes that correspond to outpatient hospital services that are expressly excluded from SNF Consolidated Billing. Hospital claims for outpatient services that are submitted with one of these excluded codes bypass the existing CWF edits, and are then sent to the appropriate Medicare Administrative Contractor for further editing and payment. Hospital claims submitted without one of these codes are denied for SNF Consolidated Billing.
The new ambulance edits will extend these process one step further. The ambulance claim will be associated with the outpatient hospital claim on the same date. To the extent that hospital claim is bundled under SNF Consolidated Billing, the associated ambulance claim will also be bundled. To the extent the hospital claim is unbundled, the associated ambulance claim will be unbundled.
In order for these new edits to work properly, there must be an outpatient hospital in Medicare’s claim history. If the ambulance claim beats the hospital claim into the system, the ambulance claim will be rejected. If and when an outpatient hospital claim with the same date of service enters Medicare’s system, the initial rejection of the ambulance claim will be overturned, and the ambulance claim will be reprocessed using the same edits.
It is important to note that the new edits were designed to reject the ambulance claim as a bundled service unless the hospital claim indicates that it should not be bundled. In other words, these edits are designed to be “over inclusive.” This over-inclusiveness creates the potential for ambulance denials in situations that, on their face, would not appear to be bundled.
A few examples will help illustrate this point. Imagine a situation where the patient elects, for whatever reason, to pay out-of-pocket for their hospital care (in a situation where that care would not be bundled to the SNF), and, as a result, the hospital does not submit a bill to Medicare for its services. Based on how the new edits are designed, your ambulance claim for the transport to that excluded service will be rejected based on the lack of a hospital claim. Or maybe the patient has both Medicare and the V.A., and has elected to have the V.A. be the primary payer for their required hospital care. Again, there would likely be no outpatient hospital claim submitted to Medicare on that date of service, resulting in the rejection of your ambulance claim.
I can see your point, but those examples are pretty far-fetched. How big an issue is this really?
I agree those examples are pretty far-fetched. However, there are other situations that create the same problem. For example, what about an emergent response to transport an SNF patient to the hospital for necessary emergency services? Imagine if you are called to respond late at night (e.g., 11:30 p.m.) tonight. Now imagine that, by the time you get to the patient, load them into the vehicle, and transport them to the ED, it has crossed over midnight into the next day.
What date of service is going to be on the hospital’s claim? Almost certainly, the hospital will use tomorrow’s date. As a result, when your claim hits Medicare’s system, there will not be an associated hospital claim, which will result in your claim being rejected as the responsibility of the SNF. In this situation, Medicare’s edit has worked as intended, but the result is the denial of a claim that should be separately payable by Medicare Part B.
Okay, I can see how this might be annoying,
but I can appeal the claim and likely win on appeal, right?
Yes and no. The problem is that you are not likely to win on either of the first two levels of appeal, as they are likely going to rely upon the information in the CWF. I can see you possibly winning your appeal at the ALJ level…5 to 7 years from now.
In other words, the appeals process is unlikely to provide an acceptable resolution. Instead, I think the majority of ambulance providers are going to look to the SNFs to make good in these situations. Of course, the SNFs are likely going to disclaim liability, arguing (correctly) that ambulance transportation to an ED is an excluded service.
This is where the agreement with the SNF comes into play. One key purpose of contracts is to allocate known risks between the parties. In this instance, the “risk” that needs to be addressed is the possibility that Medicare might incorrectly reject your claim thinking it is bundled to the SNF. I would argue that this risk should be absorbed by the SNF. The transport to the ED should have suspended the patient’s SNF stay, which would have allowed you to receive a separate payment from Medicare. However, the fact that your claim was rejected is proof positive that the CWF does not reflect the suspension of the patient’s SNF stay. Indirectly, it also serves as proof that the SNF received a per diem payment for the patient on that date. To me, the fact that they accepted the per diem payment means they accepted the risk of a bundled ambulance service on that date. I would also argue that it was their failure to properly suspend the patient’s SNF stay that set in motion your denial. Either way, I would be looking to the SNF for payment.
Based on my experience, the typical agreement with an SNF does not address this situation. Frequently, these agreements do not even address the specifics of SNF Consolidated Billing. Instead, I tend to see general language indicating that the ambulance provider will bill the SNF when payment responsibility lies with the SNF under an applicable federal or state health care program. I doubt that language is going to convince an SNF to take financial responsibility for the situation discussed above.
The good news is that your existing agreements can easily be revised to address this situation. The language I would recommend is something along the lines of:
“The parties acknowledge and agree that a denial from Medicare for SNF consolidated billing shall constitute conclusive evidence that a transportation service is the financial responsibility of the facility.”
In sum, the new SNF Consolidated Billing edits are going to increase the frequency with which we are forced to look to the SNFs for payment. In most instances, it will be a situation where the SNF is legally responsible under SNF Consolidated Billing. However, there will also be situations where the over-inclusive nature of the edits results in the claim being incorrectly denied as the SNF’s responsibility. The question becomes how you want to handle these incorrect denials. Do you want to appeal and hope CMS reverses its decision? Or do you want to hold the SNF responsible? If you want to hold the SNF responsible, you will likely need to revise your agreements with the SNFs.
Have an issue you would like to see discussed in a future Talking Medicare blog?
Please write to me at bwerfel@aol.com.

In a Member Advisory issued last week, the AAA provided an update on a series of new Common Working File (CWF) edits intended to identify ambulance transports furnished in connection with outpatient hospital services that are properly bundled to the skilled nursing facility under the SNF Consolidated Billing regime. These new edits are set to go into effect on April 1, 2019.
In our discussion of the implementation specifics, we attempted to answer the question of what would happen when an ambulance claim is submitted prior to the receipt of the associated hospital outpatient claim, and where the associated hospital claim eventually hit Medicare’s system. Specifically, we indicated as follows:
“The Transmittal contains further instructions that the CWF be updated to identify previously rejected ambulance claims upon receipt of an associated hospital claim for the same date of service that contains an Exempted Code. Once identified, the Shared System Maintainer (SSM) is supposed to adjust the previously rejected or denied ambulance claim. At this point, the nature of that “adjustment” is unclear, i.e., it is unknown whether the SSM will automatically reprocess the ambulance claim for payment. The AAA is seeking additional clarification from CMS on this important point.”
On March 15, 2019, CMS responded to our request for clarification. Specifically, CMS indicated that it has instructed the SSM and/or its Medicare Administrative Contractor (MAC) to automatically reprocess claims that were rejected for lack of an associated hospital outpatient claim.
Upon reprocessing, the claims will pass the edits to the extent the associated hospital claim contains a HCPCS or CPT code that indicates that the hospital outpatient service was excluded from SNF Consolidated Billing. Such claims would then be forwarded to the MAC for further editing, and either paid or denied. By contrast, when the associated hospital outpatient claim contains HCPCS or CPT codes that suggest the hospital services should be bundled to the SNF, the claim will be reprocessed and denied by the MAC with a remittance advice code indicating that the SNF is financially responsible.
March 27, 2019 | 2:00 PM Eastern
Speakers: Brian Werfel, Esq.
$99 for Members | $198 for Non-Members
Join AAA Medicare Consultant Brian Werfel, Esq., to go over the new SNF Consolidated Billing edits that go into effect April 1, 2019. These edits are being implemented by CMS in response to 2017 investigation by the HHS Office of the Inspector General that determined that CMS lacked the appropriate claims processing edits to properly identify ambulance transports provided in connection with hospital outpatient services that are not expressly excluded from SNF PPS. The implementation of these new edits will force ambulance providers and suppliers to rethink their current claims submission processes for SNF residents. Ambulance providers and suppliers will need to make a decision on what to do with these claims moving forward. Sign up today to make sure your service is ready!
On November 2, 2018, the Centers for Medicare and Medicaid Services (CMS) issued Transmittal 2176 (Change Request 10955), which would establish a new series of Common Working File (CWF) edits intended to identify ambulance transports furnished in connection with outpatient hospital services that are properly bundled to the skilled nursing facility under the SNF Consolidated Billing regime. These new edits are set to go into effect on April 1, 2019.
In 2017, the HHS Office of the Inspector General conducted an investigation of ground ambulance claims that were furnished to Medicare beneficiaries during the first 100 days of a skilled nursing home (SNF) stay. Under the SNF Consolidated Billing regime, SNFs are paid a per diem, case-mix-adjusted amount that is intended to cover all costs incurred on behalf of their residents. Federal regulations further provide that, with limited exceptions, the SNF’s per diem payment includes medically necessary ambulance transportation provided during the beneficiary’s Part A stay. The OIG’s report was issued in February 2019.
The OIG conducted a review of all SNF beneficiary days from July 1, 2014 through June 30, 2016 to determine whether the beneficiary day contained a ground ambulance claim line. The OIG excluded beneficiary days where the only ambulance claim line related to: (1) certain emergency or intensive outpatient hospital services or (2) dialysis services, as such ambulance transportation would be excluded from SNF Consolidated Billing. The OIG determined that there were 58,006 qualifying beneficiary days during this period, corresponding to $25.3 million in Medicare payments to ambulance suppliers.
The OIG then selected a random sample of 100 beneficiary days for review. The OIG determined that 78 of these 100 beneficiary days contained an overpayment for the associated ambulance claims, as the services the beneficiary received did not suspend or end their SNF resident status, nor was the transport for dialysis. The OIG determined that ambulance providers were overpaid a total of $41,456 for these ambulance transports. The OIG further determined that beneficiaries (or their secondary insurances) incurred an additional $10,723 in incorrect coinsurance and deductibles.
Based on the results of its review, the OIG estimates that Medicare made a total of $19.9 million in Part B overpayments to ambulance suppliers for transports that should have been bundled to the SNFs under SNF Consolidated Billing regime. The OIG estimated that beneficiaries (and their secondary insurances) incurred an additional $5.2 million in coinsurance and deductibles related to these incorrect payments.
The OIG concluded that the existing edits were inadequate to identify ambulance claims for services associated with hospital outpatient services that did not suspend or end the beneficiary’s SNF resident status, and which were not related to dialysis. The OIG recommended that CMS implement additional edits to identify such ambulance claims.
In response to the OIG’s report, CMS issued Transmittal 2176, which implements a new series of claims processing edits to identify ambulance claims associated with outpatient hospital services that should be bundled to the SNF. As noted above, these edits will go into effect on April 1, 2019.
These new claims processing edits are somewhat complicated. In order to properly understand how these claims edits will work, it is helpful to understand that CMS already has claims processing edits in place to identify hospital outpatient claims that should be bundled to the SNF. These CWF edits operate by referencing a list of Healthcare Common Procedure Coding System (HCPCS) or Current Procedural Terminology (CPT) codes that correspond to outpatient hospital services that are expressly excluded from SNF Consolidated Billing. Hospital claims for outpatient services that are submitted with one of these excluded codes bypass the existing CWF edits, and are then sent to the appropriate Medicare Administrative Contractor for further editing and payment. Hospital claims submitted without one of these codes are denied for SNF Consolidated Billing. For convenience, the list of HCPCS and CPT codes excluded from SNF Consolidated Billing is hereinafter referred to as the “Exempted Codes.”
The new edits for ambulance claims will compare Part B ambulance claims to the associated outpatient hospital claim to see whether or not that hospital claim is excluded from SNF Consolidated Billing.
Under these new edits, the CWF will reject an incoming ambulance claim whenever the beneficiary is determined to be in an SNF Part A stay if either:
When an incoming ambulance claim is rejected by the CWF, it will be sent to the applicable Medicare Administrative Contractor and rejected (Part A Ambulance Providers) or denied (Part B Ambulance Suppliers) using the applicable Claim Adjustment Reason Code/Remittance Advice Remark Code for SNF Consolidated Billing. In other words, the ambulance claim will be denied with an indication that youshould bill the SNF.
The Transmittal contains further instructions that the CWF be updated to identify previously rejected ambulance claims upon receipt of an associated hospital claim for the same date of service that contains an Exempted Code. Once identified, the Shared System Maintainer (SSM) is supposed to adjust the previously rejected or denied ambulance claim. At this point, the nature of that “adjustment” is unclear, i.e., it is unknown whether the SSM will automatically reprocess the ambulance claim for payment. The AAA is seeking additional clarification from CMS on this important point.
Based on the current experience of hospital providers, the AAA is cautiously optimistic that the new edits can be implemented in a way that proper identifies ambulance transports associated with hospital outpatient claims that should be bundled to the SNF vs. those that correctly remain separately payable by Medicare Part B.
However, the AAA has some concerns with the manner in which CMS intends to apply these edits. Ambulance providers and suppliers are typically in a position to submit their claims earlier than the corresponding hospital, many of which submit claims on a biweekly or monthly cycle. This creates a potential timing issue. This timing issue arises because the edits will reject any ambulance claim that is submitted without an associated hospital claim on file. In other words, even if the hospital outpatient service is properly excluded from SNF Consolidated Billing, the ambulance claim will still be rejected if it beats the hospital claim into the system. The hope is that CMS will subsequently reprocess the ambulance claim once the hospital claim hits the system. However, at this point in time, it is unclear whether these claims will be automatically reprocessed, or whether ambulance providers and suppliers will be forced to appeal these claims for payment.
One option available to ambulance providers and suppliers would be to hold these claims for a period of time, in order to allow the hospitals to submit their claims. By waiting for the hospital to submit its claim, you can ensure that your claims will not be denied solely due to the timing issue. This should eliminate the disruption associated with separately payable claims being rejected and then subsequently reprocessed and/or appealed. It would also give you a degree of certainty when billing the SNF for claims that are denied for SNF Consolidated Billing. However, holding claims carries an obvious downside, i.e., it will disrupt your normal cash flow.
To summarize, the implementation of these new edits will force ambulance providers and suppliers to rethink their current claims submission processes for SNF residents. Ambulance providers and suppliers will need to make a decision on whether to hold claims to minimize the potential for problems, or to continue their existing submission practices and deal with any issues as they arise.
AAA webinar on new SNF Consolidated Billing edits
March 27, 2019 | 2:00 PM Eastern
Speakers: Brian Werfel, Esq.
$99 for Members | $198 for Non-Members
Join AAA Medicare Consultant Brian Werfel, Esq., to go over the new SNF Consolidated Billing edits that go into effect April 1, 2019. These edits are being implemented by CMS in response to 2017 investigation by the HHS Office of the Inspector General that determined that CMS lacked the appropriate claims processing edits to properly identify ambulance transports provided in connection with hospital outpatient services that are not expressly excluded from SNF PPS. The implementation of these new edits will force ambulance providers and suppliers to rethink their current claims submission processes for SNF residents. Ambulance providers and suppliers will need to make a decision on what to do with these claims moving forward. Sign up today to make sure your service is ready!
On October 1, 2018, CMS implemented an additional thirteen (13%) cut in reimbursement for non-emergency BLS transports to and from dialysis. This cut in reimbursement was mandated by Section 53108 of the Bipartisan Budget Act of 2018. This on top of a ten (10%) cut in reimbursement for dialysis transports that went into effect on October 1, 2013. As a result, BLS non-emergency ambulance transports to and from dialysis that occur on or after October 1, 2018 will be reimbursed at 77% of the applicable Medicare allowable.
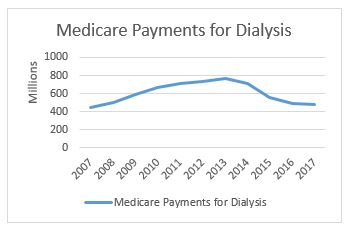
In related news, CMS has released its national payment data for calendar year 2017. This data shows a continued reduction in total Medicare payments for dialysis transports. Medicare paid $477.7 million on dialysis transports in 2017, down from $488.9 million in 2016. This continues a downward trend that has seen total payments decline from a high of more than $750 million in 2013 (see accompanying chart to the right). Not coincidentally, it was in 2013 that our industry saw its first reduction in Medicare’s payments for dialysis transports.
The payment reduction is partially the result of the reduction in the amounts paid for dialysis services. However, it is also reflective of an overall decline in the number of approved dialysis transports. For this, we can look primarily to the impact of a four-year demonstration project that requires prior authorization of dialysis transports in 8 states and the District of Columbia.
As a reminder, the original prior authorization states were selected based on higher-than-average utilization rates and high rates of improper payment for these services. In particular, the Medicare Payment Advisory Commission (MedPAC) had singled out these states as having higher-than-average utilization of dialysis transports in a June 2013 report to Congress. The chart below shows total spending on dialysis in those states in the years immediately preceding the implementation of the prior authorization project up through 2017, the third year of the demonstration project. While the three states had very different trajectories prior to 2015, each showed a significant decrease in total payments for dialysis under the demonstration project.
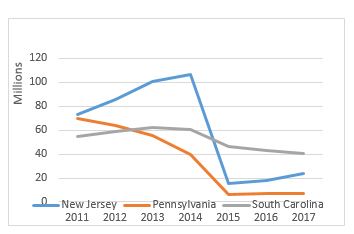
However, it is the trajectory of these changes that I want to discuss in this month’s blog. In previous blogs, I discussed the impact of the particular Medicare Administrative Contractor on the outcomes under prior authorization. Specifically, I noted that, while dialysis payments dropped in each state, the decline was far more dramatic in the states administered by Novitas Solutions (NJ, PA) than in the South Carolina, which was administered by Palmetto GBA. This trend continued in the second year of the program, which saw prior authorization expanded into five additional states and the District of Columbia. Those states administered by Novitas (DE, MD) saw far greater declines than the states administered by Palmetto (NC, VA, WV).
Given these declines, the data from the third year is somewhat surprising. The states administered by Palmetto continued to see declines in total dialysis payments, with the only exception being West Virginia. However, in the states administered by Novitas, we saw total dialysis payments increase, particularly in New Jersey, which saw nearly a 33% increase in total dialysis payments.
Three years into the prior authorization program, it is starting to become clear that the two MACs have approached the problem of overutilization of dialysis transports using two different approaches. Palmetto appears to have adopted a slow-and-steady approach, with total payments declining in a consistent manner year after year. By contrast, Novitas adopted more of a “shock the system” approach, where it rejected nearly all dialysis transports in the first year, and has adopted a somewhat more lenient approach in subsequent years.
Last year, I wrote that two years of data under the prior authorization program permitted two conclusions: (1) the implementation of a prior authorization process in a state will undoubtedly result in an overall decrease in the total payments for dialysis within that state and (2) the size of that reduction appears to be highly dependent on the Medicare contractor.
With an additional year of data, I think both conclusions remain valid, although I would revise the second to suggest that the initial reduction has more to do with the Medicare contractor. The evidence from the third year of the program suggests that the trends tend to equalize after the first few years. It is also possible that Novitas felt a more aggressive approach was needed in the first few years to address evidence of widespread dialysis overutilization in the Philadelphia metropolitan area.
This has potential implications beyond the demonstration project, as CMS looks towards a possible national expansion of the program. Among other issues, it suggests that the AAA must continue its efforts to work with CMS and its contractors on developing more uniform standards for coverage of this patient population.
The AAA continues to work on legislation that would restructure this cut to dialysis transport reimbursement. The AAA strongly supports the NEATSA Act (H.R.6269) introduced by Congressman LaHood (R-IL) and Congresswoman Sewell (D-AL) that would restructure the offset so that a majority of the additional reduction would be focused on those ambulance service agencies in which 50% or more of their volume are repetitive BLS nonemergency transports. AAA members and the AAA are working to get a Senate companion bill introduced shortly. The goal of this legislation would be to have the restructured offset go into effect as soon as possible. Thank you to the dozens of AAA members who have already contacted their members of Congress voicing their support for this critical legislation.
Have an issue you would like to see discussed in a future Talking Medicare blog? Please write to me at bwerfel@aol.com

The Office of the Inspector General released its report “Medicare Improperly Paid Providers for Non Emergency Ambulance Transports to Destinations Not Covered by Medicare“.
In sum, the OIG reviewed claims that Medicare paid for 2014 – 2016 non-emergency ambulance transports. The review focused on transports to non-covered destinations. OIG found that $8,633,940 was paid by Medicare for non-emergency ambulance transports under codes A0425 (ground mileage), A0426 (ALS non-emergency) and A0428 (BLS non-emergency) during this period of time.
The review was based solely on the claims and not based on a medical review or interviews of providers.
The claims that should not have been paid were to the following destinations:
OIG recommended (and CMS agreed) that CMS:
There is a chart in the report that indicates the improper payments for each jurisdiction. It is interesting to note that the overpayments range from a low of $515 (First Coast) to a high of $5,006,696 (Cahaba).
The report can be obtained at: https://go.usa.gov/xU5vf
On April 13, 2018, CMS released two Transmittals, Transmittal 243 and Transmittal 4021, and a related MedLearns Matter Article (MM10550). Collectively, these documents clarify Medicare’s coverage of ambulance transportation of SNF residents in a stay not covered by Part B, but who have Part B benefits, to the nearest supplier of medically necessary services that are not available at the SNF. This clarification relates to both the ambulance transport to the site of medical care, and the return trip.
In order to properly understand the clarification, it is helpful to review Medicare’s coverage of ambulance transportation provided to SNF residents. At the onset, it is important to note that Medicare draws a distinction between the first 100 days of a beneficiary’s SNF stay, and any subsequent days of the same stay. The first 100 days are commonly referred to as the “Part A Period.” Under current Medicare rules, all ambulance transportation provided during the Part A Period is the financial responsibility of the SNF, unless a specific exemption applies. Outside the Part A Period, Medicare’s coverage rules generally mirror the rules applicable to ambulance transports that originate at the patient’s residence. However, there is an exception that relates to transportation to and from therapeutic or diagnostic sites (i.e., those facilities identified with the “D” modifier). This clarification relates to transportation to and from diagnostic sites.
Medicare rules are clear that transportation of an SNF resident outside the Part A Period for the purpose of receiving medically necessary care that could not be provided at the SNF will be covered to the extent the ambulance transportation was both medically reasonable and necessary. This is true regardless of the type of facility to which the patient is transported. In this context, the term “reasonable” refers to the costs of transporting the patient to the site of medical care. Where it is cheaper to bring the patient to the service (e.g., an MRI or CT scan), Medicare will cover the service. Where it is cheaper to bring the service to the patient (e.g., certain minor procedures), Medicare rules indicate that the transportation would not be covered.
In other words, once an SNF resident is outside the Part A Period, Medicare will cover a medically necessary ambulance transport to a diagnostic site provided that it is cheaper to transport the patient to that site than to transport the equipment needed to provide care to the SNF.
As you can imagine, determinations as to the reasonableness of a particular service can be quite subjective. Moreover, these determinations can typically only be made on a case-by-case basis, i.e., it is extremely difficult for Medicare Administrative Contractors to make such decisions without seeing the ambulance trip report and other supporting documentation. As a result, CMS has historically given its MACs broad discretion to make these determinations.
The MACs have elected to utilize this discretion in various ways. Some MACs have essentially elected to rely upon the ambulance provider to make such determinations prior to submitting the claims. These MACs have therefore elected not to implement front-end edits for such claims.
Other MACs have elected to issue an initial denial, and handle reasonableness determinations through the appeals process. These MACs do so by implementing edits into their claims processing system that automatically deny claims submitted with the “ND” modifiers. However, because Medicare coverage rules indicate that transportation from anywhere to an SNF may be covered, these MACs do not have a corresponding edit to deny claims submitted with the “DN” modifiers.
The result is various inconsistencies in the ways claims for these situations are handled. Depending on the MAC jurisdiction in which you operate, a claim for an ambulance transport from an SNF to a diagnostic site (“ND”) for a beneficiary outside the Part A Period may be paid or denied. For those of you that operate in jurisdictions where the MAC denies this claim, you may also see the return trip either paid or denied. Note: if the transportation to the diagnostic site is denied as not being “reasonable,” the return trip should be denied as well.
It is these inconsistencies that CMS is addressing. Essentially, CMS is instructing those MACs that use claims processing edits to deny the “ND” transport to remove those edits. The practical effect is to force the MACs to use some other criteria to determine whether the roundtrip is reasonable (and, therefore, covered by Medicare Part B).
Please note that the coverage rules and clarification summarized above applies only to therapeutic and diagnostic facilities. It does not apply to ambulance transportation to and from a physician’s office. With the narrow exception of emergency ambulance transportation to a physician’s office as an interim stop on the way to a hospital, such transportation has always been and remains a non-covered service.
While I believe the change is, on net, a positive one for the industry, I would caution against reading too much into this clarification. CMS is not indicating that these transports will be covered in all instances. CMS is simply saying that, with respect to the initial processing of claims, it is willing to sacrifice some potential accuracy for the sake of greater national consistency. CMS in not restricting its MACs from using other means to make reasonableness determinations, e.g., the use of development requests, prepayment review, etc. While it is reasonable to assume that most MACs will elect not to utilize these tools, only time will tell if that is indeed what comes to pass. In the meantime, I am going to enjoy one of those rare instances where CMS used common sense, and removed an additional burden on our industry.
Have an issue you would like to see discussed in a future Talking Medicare blog?
Please write to me at bwerfel@aol.com.

The AAA would like to take this opportunity to update members on a number of issues related to Medicare reimbursement:
Have any questions about these updates? Contact Brian Werfel at bwerfel@aol.com

CMS held its latest Open Door Forum on Wednesday, March 7, 2018. As with past Open Door Forums, CMS started the call with the following series of announcements:
Medicare Fee Schedule – CMS indicated that the Bipartisan Budget Act of 2018, enacted on February 9, 2018, contained several provisions that impacted the payment of ambulance claims under the Medicare Ambulance Fee Schedule:
Temporary Enrollment Moratorium – CMS indicated that the temporary moratorium on the enrollment of new ground non-emergency ambulance providers in Texas was lifted on September 1, 2017. CMS further indicated that the enrollment moratorium was extended for the states of New Jersey and Pennsylvania for an additional six months on January 29, 2018. CMS will need to make a determination on or before July 29, 2018 on whether to lift the moratorium or extent it for an additional six months in that state.
Following the announcements, CMS moved into a brief Question & Answer period. Most of the questions were not answered on the call; instead, CMS took the contact information of the person asking the question, and indicated that they would respond directly to them at a later date. However, the following questions were answered:
Have questions? Please write to the Werfels at bwerfel@aol.com.

Novitas Solutions, Inc. recently announced that it will no longer issue prior authorizations for scheduled, repetitive non-emergency transports, effective December 1, 2017. This announcement was based on Novitas’ expectation that the demonstration project will expire at the end of this calendar year. For ambulance suppliers in the states that currently operate under prior authorization, the focus invariably turns to what that means for their repetitive patient populations?
First a little background. In May 2014, CMS announced the implementation of a three-year prior authorization demonstration project for repetitive scheduled non-emergency ambulance transports. This demonstration project was initially limited to the states of New Jersey, Pennsylvania, and South Carolina. These states were selected based on higher-than-average utilization rates and high rates of improper payment for these services. In particular, the Medicare Payment Advisory Commission (MedPAC) had singled out these states as having higher-than-average utilization of dialysis transports in a June 2013 report to Congress. As initially conceived, the prior authorization demonstration project first went into effect on December 15, 2014.
Congress subsequently elected to expand this demonstration project to additional states as part of the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA). Specifically, Congress mandated that the program be expanded to six additional states (Delaware, Maryland, North Carolina, Virginia, and West Virginia) and the District of Columbia by January 1, 2016, and then potentially to the rest of the nation by January 1, 2017. However, CMS never issued the required report; as a result, the contemplated national expansion never occurred.
If you operate in a state that is not currently operating under prior authorization, the answer to this question is relatively straightforward, i.e., nothing will change.
If, however, operate in a state that is currently subject to prior authorization, this question is a bit trickier. What we do know is that the actual mechanics of submitting claims will revert to the same process you experienced prior to the implementation of prior authorization. You will submit claims for repetitive patients directly to the Medicare Administrative Contractor (MAC), who will likely process them in same manner they process other Medicare claims. In other words, 14 days after the submission of the claim, you will likely receive a remittance notice indicating that the claim has either been paid or denied.
We also know that you will no longer benefit from the protections against post-payment review of these claims. Under the prior authorization model, CMS made clear that it would not audit claims paid based on a valid authorization, except in instances where it could demonstrate that the prior authorization was fraudulently procured.
What we don’t know is whether the MACs will implement any temporary measures to guard against ongoing over-utilization and/or fraud. To better understand what I mean, put yourself in the position of the MAC. You have empirical evidence (see the chart to the right) that prior authorization has resulted in dramatic reductions in the amount of Medicare dollars paid for dialysis transports. You have further seen little evidence that this reduction in payments has resulted in any serious access to care issues.
The logical conclusion you would draw is that the amounts paid for dialysis prior to the implementation of prior authorization were likely excessive. If so, you might consider some proactive steps to prevent dialysis utilization from increasing back to the levels seen prior to the implementation of prior authorization.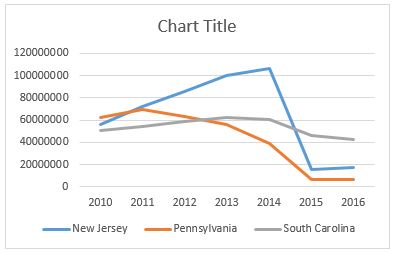
So, it is possible (perhaps even likely) that ambulance suppliers in some of these states may see their MAC elect to implement prepayment reviews for dialysis patients. This could be similar to the process Novitas used for the initial three round trip transports to dialysis.
I also think it is reasonable to expect that the MACs, the Zone Program Integrity Contractors, and the OIG will monitor utilization trends, with an eye towards conducting post-payment reviews on ambulance suppliers that see their dialysis volume increase sharply next year.
In the previous section, I touched on the steps Medicare and its contractors might take to prevent a return to pre-prior authorization levels of dialysis utilization. In this section, I want to talk about some of the knock-on effects ambulance providers are likely to see.
One of the more interesting changes we saw in the prior authorization regime was a re-balancing of the power dynamic between ambulance suppliers and facilities, i.e., assisted living facilities and skilled nursing homes. Prior to the implementation of prior authorization, that power dynamic was slanted heavily in favor of the facility. By that I mean they could exert tremendous pressure on ambulance suppliers to take marginal patients by ambulance. If you were involved in the industry prior to 2015, you undoubtedly heard an SNF administrator tell you something to the effect of “if your company won’t take the patient by ambulance, I can easily find another company that will.” In competitive markets, that statement was usually accurate.
Under the demonstration project, prior authorization or lack thereof traveled with the patient. What that meant is that if your ambulance company submitted a prior authorization request that was denied, that denial would apply to any other ambulance company that might be interested in taking the patient. As a result, the nursing home could no longer hold the threat of going elsewhere with their business over your head.
Prior authorization also affected the standing policies of dialysis centers. Many free-standing dialysis centers have standing policies that they will not assist in transferring the patient to and from the dialysis treatment chair. This meant that patients that could be transported in a wheelchair van, but who required assistance to transfer out of their wheelchair presented a conundrum. There wouldn’t be medical necessity for the ambulance, but there would be no easy way for you to transfer them into the treatment chair without a second crew member (something most wheelchair van services don’t offer). Under prior authorization, it was easier for the ambulance company to push back, since they knew they wouldn’t be paid for the ambulance. As a result, I have heard that dialysis employees in these states had started to assist patients in transferring.
No really, it’s true…
One potential consequence of the prior authorization going away is that it may shift this power dynamic back to the facilities, with all of the negative consequences that are likely to result.
“Okay, I get what you are saying, but what I really want to know is whether I should loosen our standards for accepting a dialysis patient or not?”
Good question. Unfortunately, not one that permits an easy answer. The implementation of prior authorization shifted the cost-benefit analysis associated with transporting dialysis patients. It was likely that you were going to have a smaller number of patients approved and paid, but you could rest easy that you wouldn’t be at risk of having to return that money years later as the result of a Medicare audit.
The expiration of prior authorization shifts the cost-benefit analysis yet again. It is likely that you have tightened up your criteria for who you accept for dialysis transportation as a result of prior authorization. Loosening those criteria would almost certainly result in an increase in your short-term revenues. However, that would be offset, to some degree, by the increased risk of a Medicare audit.
For that reason, the course of action I have been recommending to people is not to dramatically loosen your standards. Instead, I typically ask whether they currently have patients that they believe do require an ambulance, but who were rejected for prior authorization by the MAC. Most providers respond that they do. Put another way, we are trying to identify the patients that you would feel comfortable defending in an audit. That is the additional population I would target for transportation next year.
Have an issue you would like to see discussed in a future Talking Medicare Blog? Please write to me at bwerfel@aol.com.
On September 14, 2017, CMS held its latest Open Door Forum. As usual, it started with a few announcements, as follows:
Support Extending the Medicare Add-ons!
Following these announcements, a Q & A period ensued. Most of the questions were not answered on the call, other than to advise the caller to submit their question via e-mail and CMS will respond to their concern via e-mail or to contact their Medicare Administrative Contractor.
Two items of note in the Q & A were as follows:
Have questions? Please write to the Werfels at bwerfel@aol.com.

Every year, CMS releases data on aggregate Medicare payments for the preceding year. This file is referred to as the Physician/Supplier Procedure Master File (PSP Master File). This past month, CMS released the 2016 PSP Master File, which contains information on all Part B and DME claims processed through the Medicare Common Working File with 2015 dates of service.
In September’s blog post, I discussed the results of the first year of the prior authorization demonstration project for repetitive, scheduled non-emergency ground ambulance transports. During this first year, the project was limited to three states: New Jersey, Pennsylvania, and South Carolina. The data confirms that these three states saw a dramatic reduction in Medicare’s approved payments for dialysis transports.
This month, I will be discussing the national payment trends for non-emergency ground ambulance transports, and, in particular, Basic Life Support non-emergencies.
In 2015, Medicare paid approximately $990 million for BLS non-emergency transports. This is 13% less than what it paid for BLS non-emergency transports in 2014 ($1.14 billion). Please note that these figures only reflect payments for the base rate; when the payments for the associated mileage are included, the reduction is even more dramatic.
In actual terms, this means Medicare Administrative Contractors (MACs) approved nearly 1 million fewer BLS non-emergency transports in 2015 (5.86 million) than they approved in 2014 (6.81 million). Roughly 75% of this reduction can be directly attributed to the prior authorization program in the three states listed above. Note: the reduction in approved dialysis transports in New Jersey accounts for nearly half of the national decline). However, that leaves nearly 250,000 fewer approved transports in the remaining 47 states. This reduction was not the result of fewer claims being submitted in 2015; the number of submitted claims was actually higher in 2015 than 2014. Rather, the data shows that this reduction is the result of the MACs actively denying many more claims than in year’s past.
I believe these reductions are the direct result of a step-up in the enforcement activities of the MACs, which I also believe has the tacit, if not outright, approval of CMS.
To test this thesis, I looked at the state-by-state data to see if any trends could be found. What I found was that 28 states saw increases in the total number of approved BLS non-emergency transports in 2015, with 19 states seeing decreases. However, on its face, that number is somewhat deceiving. The states that saw increases tended: (1) to see either relatively small increases or (2) had relatively low utilization rates to begin with. The states that saw decreases tended to be larger states with higher utilization rates, and those decreases tended to be larger in percentage terms. For instance, California saw a 21.5% decrease in the number of approved BLS non-emergency transports. Ohio saw an 11.7% decrease.
Digging deeper, it becomes clear that a state’s overall change in payments for BLS non-emergencies is almost perfectly correlated with its change in payments for dialysis transports. In other words, to the extent the state saw an overall reduction in payments for BLS non-emergencies, that reduction – – in nearly all cases – – was the result of the total payments for dialysis decreasing by more than any offsetting increase in the total payments for non-dialysis transports.
These relative changes in dialysis were also highly correlated with the MAC that administers Medicare claims in that state. To the extent your state saw a reduction in dialysis payments, it is highly likely that neighboring states administered by the same MAC saw similar reductions in payments. The following charts will help illustrate this point:
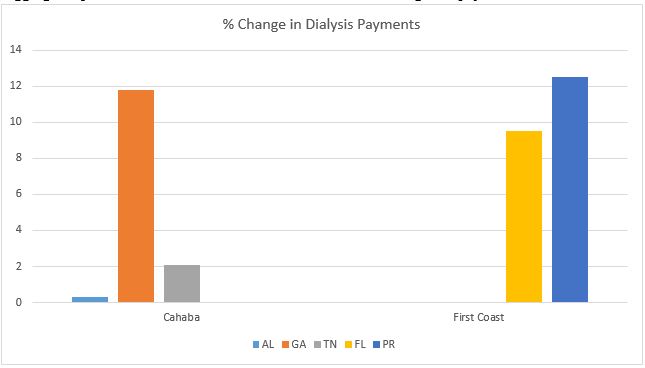 As you can see, all three states within Cahaba’s jurisdiction saw a net increase in the total payments for dialysis. While the increases themselves were quite minor in Alabama and Tennessee, Georgia saw an 11.8% increase in total payments for dialysis. Similarly, both Florida and Puerto Rico saw significant increases in the approved payments for dialysis.
As you can see, all three states within Cahaba’s jurisdiction saw a net increase in the total payments for dialysis. While the increases themselves were quite minor in Alabama and Tennessee, Georgia saw an 11.8% increase in total payments for dialysis. Similarly, both Florida and Puerto Rico saw significant increases in the approved payments for dialysis.
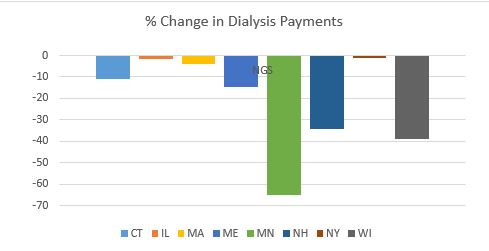
By contrast, every state in National Government Services’ (NGS’) jurisdiction with more than 1,000 paid dialysis transports in 2015 saw a net reduction in the total payments for dialysis. These reductions ranged from a relatively minor reduction of 1.17% in New York to a nearly two-thirds (64.58%) reduction in Minnesota.
 This trend was present in all remaining jurisdictions, although the results were more mixed. For example, with the exception of South Carolina, the three remaining states administered by Palmetto all saw increases. Likewise, the majority of states administered by WPS saw decreases. This included Indiana, which has a sizeable dialysis population. Among WPS states, only Missouri saw a small (3.90%) increase.
This trend was present in all remaining jurisdictions, although the results were more mixed. For example, with the exception of South Carolina, the three remaining states administered by Palmetto all saw increases. Likewise, the majority of states administered by WPS saw decreases. This included Indiana, which has a sizeable dialysis population. Among WPS states, only Missouri saw a small (3.90%) increase.
California saw a 31.76% decrease in its payments for dialysis. The only other Noridian states with more than 1,000 paid dialysis trips were Hawaii and Washington, which both saw increases.
Novitas presents a more complicated picture, with several large states, such as Texas, seeing double-digit increases in payments for dialysis, while other large states saw sizeable decreases.
All in all, the data suggests that CMS and its contractors continue to pay close attention to the non-emergency side of our business, particularly BLS non-emergency transports. These transports have been under scrutiny for many years, as reports from the Office of Inspector General, the Government Accountability Office and other federal agencies have flagged this portion of our industry as being particularly prone to overutilization (and, in some cases, outright fraud). However, this heightened scrutiny is not being uniformly applied across-the-board. The data suggests that certain MACs have been far more aggressive in targeting these sorts of trips across their entire jurisdictions, while others seem content to target specific (typically large) states within their jurisdictions. This could serve as a template for how MACs will approach prior authorization in their jurisdictions.
‘Praemonitus, Praemunitus’
Latin Proverb, loosely translated to “forewarned is forearmed.”
On May 13, 2016, the Government Accountability Office (GAO) publicly released a report on the comparative effectiveness of the various audit programs used by the Centers for Medicare and Medicaid Services (CMS) and its various contractors. This report was requested by Senator Orrin Hatch, the Chairman of the Senate Finance Committee, who had asked the GAO to examine: (1) the differences between prepayment and postpayment reviews and the extent to which CMS contractors utilize each, (2) the extent to which contractors focus their reviews on particular types of claims, and (3) CMS’ cost per review, and the amount of improper payments identified by contractors for each dollar they are paid.
To briefly summarize the GAO’s findings:
The GAO made two specific recommendations. First, it recommended that CMS seek legislation that would permit its RACs to conduct prepayment claims reviews. Second, it recommended that CMS develop written guidance on how its MACs should calculate the savings attributable to prepayment claims reviews. CMS disagreed with the first recommendation, believing it unnecessary in light of other programs intended to move CMS away from “pay and chase”, including prior authorization and enhanced provider enrollment screening. CMS agreed with the second recommendation.
For the years 2013 – 2014, the GAO found that the RACs focused primarily on hospital inpatient claims. For example, the GAO found that 78% of the FY 2013 claims reviewed by the RACs were hospital inpatient claims. While this number declined to 47% in FY 2014, that decline was largely attributable to CMS, under its own authority and subsequent legislation, prohibiting the RACs from reviewing certain inpatient stays during the first part of FY 2014. If you look only at postpayment reviews, the numbers were even higher, 87% in FY 2013 and 64% in FY 2014.
So why were the RACs focused on hospital inpatient claims, largely to the exclusion of other types of claims? The GAO believes the answer lies in how the RACs are compensated for their work. Recall that the RACs are paid contingency fees (of between 9% – 17.5%) based on the amount of the recovered overpayments. Given this fee structure, the GAO believed it was logical for the RACs to focus on claims with higher average dollar amounts per claim. The following chart shows the average amount of the improper payment identified by the RACs on a per-claim basis:

As you can see, the average overpayment for an inpatient hospital claim was more than $3,000 in FY 2013, compared with slightly more than $300 for a physician (or ambulance) claim. Assuming a 10% contingency fee, this means the RAC could expect to receive $300 for each inpatient hospital claim it reviewed, compared with $30 for a physician claim. Given these financial incentives, the RACs decision to focus on inpatient hospital claims makes sense.
In contrast to the RACs, the Medicare Administrative Contractors focused their program integrity activities almost exclusively on prepayment reviews. The following chart shows the breakdown of MAC reviews by provider type:

As you can see, the MAC largely focused on physician and DME claims, with physician claims (including ambulance claims) accounting for 49% of MAC reviews in FY 2013 and 55% of MAC reviews in FY 2014.
The efficacy of these reviews is unclear. This is largely due to the failure by CMS to collect consistent data on the savings from prepayment claims denials. At least 3 MACs failed to provide data on the specific funds they spent on prepayment and postpayment reviews. Instead, these MACs reported their costs as part of their broader claims processing activities. MAC also used different methods for calculating the savings from prepayment reviews. For example, 2 MACs used the billed amounts by providers to calculate total savings from denied claims, despite the Medicare allowables being significantly lower than the amounts normally billed by providers. 9 MACs used the total Medicare allowable, without differentiating between Medicare’s payment and the payments made by secondary insurers and/or patients. The remaining 5 MACs compared denied claims to similar claims that were paid to estimate what Medicare saved on claims denied as part of prepayment reviews.
The key finding in this report is the GAO’s belief that prepayment reviews are generally more cost-effective in preventing improper Medicare payments. The GAO believes this is because prepayment reviews “limit the need to recover overpayments through the “pay and chase” process, which requires administrative resources and is not always successful.”
While the GAO and CMS are in agreement that Medicare should move away from postpayment reviews, they appear to disagree on how, exactly, to implement that transition. The GAO’s report makes clear its belief that CMS should devote greater resources to prepayment reviews, with the GAO specifically recommending that CMS seek legislative authority to empower its RACs to take a greater role in conducting prepayment reviews. By contrast, CMS appears to favor prior authorization programs.
Only time will tell which of these views gains prominence. In the meantime, ambulance providers and suppliers should expect to see the RACs take an increasing interest in our industry.
Have an issue you would like to see discussed in a future Talking Medicare blog? Submit your question!