On November 30, 2018, CMS issued Transmittal 4172 (Change Request 11031), which announced the Medicare Ambulance Inflation Factor (AIF) for calendar year 2019.
The AIF is calculated by measuring the increase in the consumer price index for all urban consumers (CPI-U) for the 12-month period ending with June of the previous year. Starting in calendar year 2011, the change in the CPI-U is now reduced by a so-called “productivity adjustment”, which is equal to the 10-year moving average of changes in the economy-wide private nonfarm business multi-factor productivity index (MFP). The MFP reduction may result in a negative AIF for any calendar year. The resulting AIF is then added to the conversion factor used to calculate Medicare payments under the Ambulance Fee Schedule.
For the 12-month period ending in June 2018, the federal Bureau of Labor Statistics (BLS) has calculated that the CPI-U has increased 2.9%. CMS further indicated that the CY 2019 MFP will be 0.6%. Accordingly, CMS indicated that the Ambulance Inflation Factor for calendar year 2019 will be 2.3%.
On November 30, 2018, CMS issued a notice on its website that it would be extending the prior authorization demonstration project for another year. The extension is limited to those states where prior authorization was in effect for calendar year 2018. The affected states are Delaware, Maryland, New Jersey, North Carolina, Pennsylvania, South Carolina, Virginia and West Virginia, as well as the District of Columbia. The extension will run through December 1, 2019.
CMS indicated that the extension will provide it with an additional year to evaluate the prior authorization program, and to determine whether the program meets the statutory requirements for nationwide expansion under the Medicare Access and CHIP Reauthorization Act of 2015.
Happy National Rural Health Day! Thank you to all of the ambulance service providers who work hard providing life-saving treatment in rural areas every day.
In part of our ongoing advocacy efforts, the AAA sent a letter today to the Rural Caucuses in the United States Senate and House of Representatives. Addressed to leadership of the caucuses, Sen. Pat Roberts (R-KS), Sen. Heidi Heitkamp (D-ND), Rep. Adrian Smith (R-NE), and Rep. Tim Walz (D-MN), this in-depth letter highlights the critical work that our members do every day around the country and raises important issues affecting the industry. Issues covered in the letter include:
Stabilizing the Ambulance Fee Schedule
Make the add-ons permanent and build them into the base rate
Use new data from the ambulance cost collection program to ensure reimbursement is adequate going forward
New data should be used to assess the problems with the current ZIP-code methodology for determining rural and super-rural services
Ambulance Fee Schedule Reform
Proposed alternative models for rural ambulance services
Encouraging Congress to look at alternative destination options for ambulance service providers
Recognizing Ambulance Services as Providers of Health Care
Moving non-fire-based ambulance services from suppliers to providers under Medicare
The letter also highlights some of the burdensome regulations facing ambulance service providers that the AAA has recommended Congress address through its Red Tape initiative. These include:
Removing Unnecessary Regulatory Burdens:
Reduce the burdens created by the Physician Certificate Statement
Simplify the 855B Ambulance Enrollment Form
Address burdensome requirements of the patient signature on claims and the strict application of the revocation of billing authority
This letter from the AAA to Congressional leaders is just one part of the AAA’s ongoing effort to educate Congress on the crucial role ambulance service providers play in America’s healthcare system. The AAA wants Congress to know that in many rural areas of the country, ambulances are the medical safety net, yet face extreme challenges to staying in business thanks to below cost reimbursement and burdensome regulations. The AAA will continue to pursue this list of priorities with our members next year and going forward.
Again, Happy Rural Health Day to our members – thanks for all that you do!
If you have any questions about our letter or rural advocacy, please contact us:
Questions?: Contact Us
If you have questions about the legislation or regulatory initiatives being undertaken by the AAA, please do not hesitate to contact a member of the AAA Government Affairs Team.
Tristan North – Senior Vice President of Government Affairs tnorth@ambulance.org | (202) 802-9025
Ruth Hazdovac – AAA Senior Manager of Federal Government Affairs rhazdovac@ambulance.org | (202) 802-9027
Aidan Camas – Manager of State & Federal Government Affairs acamas@ambulance.org | (202) 802-9026
Thank you for your continued membership and support.
The American Ambulance Association is pleased to announce the publication of its 2017 Medicare Payment Data Report. This report is based on the Physician/Supplier Procedure Summary Master File. This report contains information on all Part B and DME claims processed through the Medicare Common Working File and stored in the National Claims History Repository.
The report contains an overview of total Medicare spending nationwide in CY 2017, and then a separate breakdown of Medicare spending in each of the 50 states, the District of Columbia, and the various other U.S. Territories.
For each jurisdiction, the report contains two charts: the first reflects data for all ambulance services, while the second is limited solely to dialysis transports. Each chart lists total spending by procedure code (i.e., base rates and mileage). For comparison purposes, information is also provided on Medicare spending in CY 2016.
Aarron Reinert President American Ambulance Association
Since I assumed the office of president last month at our Annual Conference, I have been deeply moved by the selfless actions of ambulance services across the nation as they responded to natural disasters. As always, EMS answered the call to help with humanity, efficiency, and professionalism. My thoughts are with those impacted by the recent storms as well as the thousands of EMTs and Paramedics currently helping with Hurricane Michael recovery.
Annual Conference & Trade Show
Thanks to each of you who attended, exhibited at, or sponsored this year’s impressive Annual Conference & Trade Show. We appreciate your support and participation—it could not have been such a success without you. Once again, congratulations to our AMBY and AAA award winners! I would also like to welcome our new board members and thank those who continue to serve. At the conference, I took a few minutes to share my thoughts about the future of our association. If you missed it, you can catch up via video or essay on the AAA site.
We can’t wait to see you in Nashville next November 4-6, 2019! Please check back at www.annual.ambulance.org early next year for more attendee information.
Opioids
The AAA continues to press policy initiatives with Congress and the Administration that are important to our members. The AAA is pleased to report that language we supported on grant funding for opioid protection training for first responders has passed both the House of Representatives and the Senate and is now headed to the President’s desk. The Senate passed the Opioid Crisis Response Act with a bipartisan vote of 98-1 in the last necessary needed action before being signed into law by the President. The impact of this legislation on the ambulance industry includes providing resources and training so that first responders and other key community sectors, including emergency medical services agencies, can appropriately protect themselves from exposure to drugs such as fentanyl, carfentanil and other dangerous licit and illicit drugs. The legislation also allows the Department of Labor to award grants to states that have been heavily impacted by the opioid crisis to assist local workforce boards and local partnerships in closing the gaps in the workforce for mental health care and substance use disorder.
Dialysis
The AAA is also working on legislation that would restructure the additional cuts dialysis transport reimbursement that went into effect on October 1, 2018. Congress included in the Bipartisan Budget Act of 2018 an offset to go along with the extension of the add-ons that will cut reimbursement for BLS nonemergency transports to and from dialysis centers by an additional 13%. This will be on top of the existing 10% reduction. The NEATSA Act (H.R.6269) by Congressman LaHood (R-IL) and Congresswoman Sewell (D-AL) would restructure the offset so that a majority of the additional reduction would be focused on those ambulance service agencies in which 50% or more of their volume are repetitive BLS nonemergency transports. In the Senate, Senator Bill Cassidy (R-LA) had previously agreed to drop a companion Bill. Thanks to the help of the AAA’s members in Alabama, Senator Doug Jones (D-AL) just agreed to co-sponsor this legislation with Senator Cassidy. The AAA will announce the Senate Bill number as soon as it is introduced.
Veterans Affairs
The AAA has also been working on improving the timely reimbursement of emergency ambulance services by the Department of Veterans Affairs (VA). Currently, the VA is the only major payer that does not follow the prudent layperson standard. This happens despite this standard being included in their own regulations regarding reimbursement for emergency care for veterans.
The AAA continues to work closely with Sen. John Boozman (R-AR) to get a similar Bill introduced in the Senate during the next Congress. The AAA and representatives from Maine also met with Sen. Susan Collins (R-ME) and her staff who helped include some critical language related to this issue in the Senate’s FY2019 MilCon-VA Appropriations Bill (S. 3024). The language can be found in the Senate’s Committee Report on that Bill. This is a crucial step in the right direction to ensure that our veterans receive the highest quality care and that ambulance service providers are adequately reimbursed in a timely manner.
The AAA’s data analyst estimates that since ambulance services are already covered services that there should be no score (cost) for this Bill. Additionally, if the Congressional Budget Office were to account for those claims that the VA is improperly denying, the estimated cost would be $270 million over ten years.
Cost Data Collection
The continues to work closely with Congress and the CMS on the creation and implementation of the new cost collection system for ambulance services. The AAA spent the last four years thinking about how CMS should collect data from ambulance service suppliers and providers, and how we can assist in helping services prepare and respond to the cost data survey. We’re developing material and resources to help ambulance service suppliers and providers prepare for being selected to provide their cost data. Though many of the finer specifics of the framework and data elements are still to be confirmed by CMS, the AAA has an in-depth and insider understanding of the anticipated process and elements.
For information on the AAA resources, please access the ambulance cost data collection webpage at www.ambulancereports.org. The AAA will announce new developments in the cost collection system via email. Although the possibility of your organization being selected to provide data is still a couple of years away, it’s important that you start preparing now.
At the AAA’s Annual Conference & Tradeshow last month in Las Vegas, CMS, through its contractor the RAND Corporation, convened a focus group where they selected several AAA members to talk directly with the contractor. The discussion centered around characteristics of ambulance services that matter for determining costs. The group also talked about how data is currently captured at the state and local levels, as well as how data is tracked within ambulance services. There was also a lot of discussion about the importance of standardizing data elements and not relying upon different state or local definitions, which could confound the data and make it impossible to compare costs across states. CMS is now reaching out to others in the industry for input. If you receive an email or a phone call from RAND Corporation, please respond. If you have questions about, or would like assistance with this project, please contact Tristan North at tnorth@ambulance.org.
SIREN Act
Lastly, the AAA is the working to ensure that the SIREN Act (S. 2830, H.R. 5429) which would reauthorize the Rural EMS Grant program and makes all provider types eligible to apply for these grants.
Membership Renewal Time
Membership is the fuel that powers our advocacy engine and enables us to offer the innovative benefits your service has come to rely on. If you have already renewed, please accept our most sincere thanks for your continued support. If you have not yet submitted payment for this year’s membership, I encourage you to renew online or reach out to staff at info@ambulance.org for assistance. AAA needs your support through membership to continue our industry-advancing work.
Thank you for entrusting me to serve as the president of your association. It is my pleasure to lead such a talented cadre of dedicated healthcare professionals. I wish you a happy Halloween and a wonderful holiday season.
Aarron Reinert
President
American Ambulance Association
During its October meeting, the Medicare Payment Advisory Commission (MedPAC), reviewed Medicare’s current policies related to non-urgent and emergency care, as these topics relate to the use of hospital emergency departments (EDs) and urgent care centers (UCCs). The Commission is examining this topic because the use of ED services in recent years has grown faster than that of physician offices. At the same time, the share of ED visits that are coded as high acuity has increased.
The Commission is exploring Medicare beneficiaries’ use of EDs and UCCs for non-urgent services. In addition, the Commission is analyzing ED coding to determine if the increase in coding high-acuity visits reflects real change in the patients treated in EDs. This slide deck shows the potential savings Medicare could realize if beneficiaries shift certain care to the UCC setting.
During the meeting, the staff sought feedback from Commissioners for developing next steps. This topic will likely continue to be addressed in future meetings.
From the perspective of ambulance payment reform, the observations made by the Commissioners and staff would also seem to support incorporating scope-appropriate ambulance services in the context of community paramedicine or treatment at the scene with referral. While additional work needs to be done by the ambulance community before these services can be incorporated into the Medicare reimbursement program, discussions like the one at MedPAC last week, show the importance of getting the details right so that ambulance services can be part of new payment models likely to be considered.
The American Ambulance Association is leading the effort with the Medicare program to develop appropriate models that account for the cost of providing services through sustainable reimbursement rates, rather than the use of temporary grants. We are also focused on ensuring services align with the scope of practice laws. Led by the Payment Reform and the Medicare Regulatory Committees, our efforts include regular meetings and discussions with leaders at the Centers for Medicare & Medicaid Services, as well as key Members of Congress. Follow us on Facebook and Twitter to learn more about our ongoing efforts.
Talking Medicare: CMS Implements Further Cuts in Reimbursement for Dialysis Services; Medicare Payment Data Shows Continued Reduction in Overall Spending on Dialysis Transports, but Net Increase in Dialysis Payments in Prior Authorization States
On October 1, 2018, CMS implemented an additional thirteen (13%) cut in reimbursement for non-emergency BLS transports to and from dialysis. This cut in reimbursement was mandated by Section 53108 of the Bipartisan Budget Act of 2018. This on top of a ten (10%) cut in reimbursement for dialysis transports that went into effect on October 1, 2013. As a result, BLS non-emergency ambulance transports to and from dialysis that occur on or after October 1, 2018 will be reimbursed at 77% of the applicable Medicare allowable.
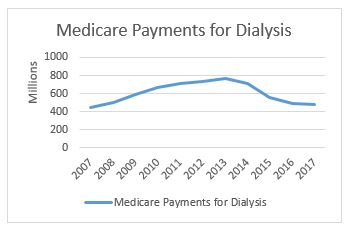
In related news, CMS has released its national payment data for calendar year 2017. This data shows a continued reduction in total Medicare payments for dialysis transports. Medicare paid $477.7 million on dialysis transports in 2017, down from $488.9 million in 2016. This continues a downward trend that has seen total payments decline from a high of more than $750 million in 2013 (see accompanying chart to the right). Not coincidentally, it was in 2013 that our industry saw its first reduction in Medicare’s payments for dialysis transports.
The payment reduction is partially the result of the reduction in the amounts paid for dialysis services. However, it is also reflective of an overall decline in the number of approved dialysis transports. For this, we can look primarily to the impact of a four-year demonstration project that requires prior authorization of dialysis transports in 8 states and the District of Columbia.
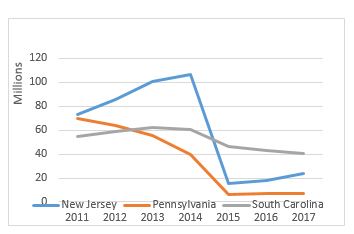
As a reminder, the original prior authorization states were selected based on higher-than-average utilization rates and high rates of improper payment for these services. In particular, the Medicare Payment Advisory Commission (MedPAC) had singled out these states as having higher-than-average utilization of dialysis transports in a June 2013 report to Congress. The chart below shows total spending on dialysis in those states in the years immediately preceding the implementation of the prior authorization project up through 2017, the third year of the demonstration project. While the three states had very different trajectories prior to 2015, each showed a significant decrease in total payments for dialysis under the demonstration project.
However, it is the trajectory of these changes that I want to discuss in this month’s blog. In previous blogs, I discussed the impact of the particular Medicare Administrative Contractor on the outcomes under prior authorization. Specifically, I noted that, while dialysis payments dropped in each state, the decline was far more dramatic in the states administered by Novitas Solutions (NJ, PA) than in the South Carolina, which was administered by Palmetto GBA. This trend continued in the second year of the program, which saw prior authorization expanded into five additional states and the District of Columbia. Those states administered by Novitas (DE, MD) saw far greater declines than the states administered by Palmetto (NC, VA, WV).
Given these declines, the data from the third year is somewhat surprising. The states administered by Palmetto continued to see declines in total dialysis payments, with the only exception being West Virginia. However, in the states administered by Novitas, we saw total dialysis payments increase, particularly in New Jersey, which saw nearly a 33% increase in total dialysis payments.
Three years into the prior authorization program, it is starting to become clear that the two MACs have approached the problem of overutilization of dialysis transports using two different approaches. Palmetto appears to have adopted a slow-and-steady approach, with total payments declining in a consistent manner year after year. By contrast, Novitas adopted more of a “shock the system” approach, where it rejected nearly all dialysis transports in the first year, and has adopted a somewhat more lenient approach in subsequent years.
Key Takeaways
Last year, I wrote that two years of data under the prior authorization program permitted two conclusions: (1) the implementation of a prior authorization process in a state will undoubtedly result in an overall decrease in the total payments for dialysis within that state and (2) the size of that reduction appears to be highly dependent on the Medicare contractor.
With an additional year of data, I think both conclusions remain valid, although I would revise the second to suggest that the initial reduction has more to do with the Medicare contractor. The evidence from the third year of the program suggests that the trends tend to equalize after the first few years. It is also possible that Novitas felt a more aggressive approach was needed in the first few years to address evidence of widespread dialysis overutilization in the Philadelphia metropolitan area.
This has potential implications beyond the demonstration project, as CMS looks towards a possible national expansion of the program. Among other issues, it suggests that the AAA must continue its efforts to work with CMS and its contractors on developing more uniform standards for coverage of this patient population.
What the AAA is Doing
The AAA continues to work on legislation that would restructure this cut to dialysis transport reimbursement. The AAA strongly supports the NEATSA Act (H.R.6269) introduced by Congressman LaHood (R-IL) and Congresswoman Sewell (D-AL) that would restructure the offset so that a majority of the additional reduction would be focused on those ambulance service agencies in which 50% or more of their volume are repetitive BLS nonemergency transports. AAA members and the AAA are working to get a Senate companion bill introduced shortly. The goal of this legislation would be to have the restructured offset go into effect as soon as possible. Thank you to the dozens of AAA members who have already contacted their members of Congress voicing their support for this critical legislation.
Have an issue you would like to see discussed in a future Talking Medicare blog? Please write to me at bwerfel@aol.com
Section 1834(l)(3)(B) of the Social Security Act mandates that the Medicare Ambulance Fee Schedule be updated each year to reflect inflation. This update is referred to as the “Ambulance Inflation Factor” or “AIF”.
The AIF is calculated by measuring the increase in the consumer price index for all urban consumers (CPI-U) for the 12-month period ending with June of the previous year. Starting in calendar year 2011, the change in the CPI-U is now reduced by a so-called “productivity adjustment”, which is equal to the 10-year moving average of changes in the economy-wide private nonfarm business multi-factor productivity index (MFP). The MFP reduction may result in a negative AIF for any calendar year. The resulting AIF is then added to the conversion factor used to calculate Medicare payments under the Ambulance Fee Schedule.
For the 12-month period ending in June 2018, the federal Bureau of Labor Statistics (BLS) has calculated that the CPI-U has increased by 2.87%.
CMS has yet to release its estimate for the MFP in calendar year 2019. However, assuming CMS’ projections for the MFP are similar to last year’s projections, the number is likely to be in the 0.5% range.
Accordingly, the AAA is currently projecting that the 2019 Ambulance Inflation Factor will be approximately 2.4%.
Cautionary Note Regarding these Estimates
Members should be advised that the BLS’ calculations of the CPI-U are preliminary, and may be subject to later adjustment. The AAA further cautions members that CMS has not officially announced the MFP for CY 2019. Therefore, it is possible that these numbers may change. The AAA will notify members once CMS issues a transmittal setting forth the official 2019 Ambulance Inflation Factor.
October Feature: Work-Life Balance and Productivity
Ten Tips for Fitting Work and Life Together
Would you like to move beyond feeling stressed or overwhelmed by your personal and work responsibilities? Or learn how to achieve personal and professional success on your own terms? “Knowing how to manage the way work and life fit together is a modern skill set we all need to succeed,” says Cali Williams Yost, an internationally recognized flexible workplace strategist and author of the books Tweak It: Make What Matters to You Happen Every Day and Work+Life: Finding the Fit That’s Right for You. Here are Yost’s 10 strategies:
Remember that work-life fit is unique for each of us. “Simply put, there is no work-life balance or perfect 5050 split between your work and your personal life,” Yost says. “If you do happen to hit a balance, you can’t maintain it because your realities are always changing, personally and professionally.” There’s also no “right way” to achieve a good work-life fit. Your goal is to find your unique, ever-changing fit, the way your work and personal realities fit together day-to-day and at major life transitions. Don’t compare yourself to others. Find the fit that’s right for you.
It’s also important to keep in mind that during major life changes — like becoming a parent, caring for an aging relative, relocating with a partner, going back to school, or easing your way into retirement — you may find yourself rethinking how you define success related to money, prestige, advancement, or caregiving. Throughout life, you may need to align and adjust your work and personal realities so they match with your vision and goals for the future.
Harness the power of small actions or “tweaks”. Even small actions can have positive and lasting effects. When you’re feeling overloaded, for example, commit to taking two or three small but meaningful steps toward a better work-life fit. Plan a long weekend away with friends. Clean out your hall closet. Take an online class to learn a new skill. Then do it again and again. Small actions can have a big impact on your sense of well-being and control. To get started, check out more than 200 small, doable get-started actions suggested by 50 work, career, and personal life experts in Yost’s book Tweak It.
Create a combined calendar and priority list. On top of a busy job and home life, how will you fit everything else into your schedule? There’s exercise, eating well, vacation, sleep, career development, time with family and friends, caregiving responsibilities, and just general life maintenance. You can’t do it all. But you can be more intentional and deliberate about how you spend your time.
First, pull together all your work and personal to-dos and priorities into one combined calendar and list. This will help you determine how you want to prioritize the tweaks — small, meaningful work, career, and personal actions and priorities — to add to your work-life fit. For example, tweaks might include planning all meals and shopping for your groceries on Sunday or getting to exercise class every Tuesday and Saturday. Or they might include researching a vacation one afternoon, going to the movies with your sister, or attending a networking event. Building actions into your schedule makes it far more likely they’ll happen. And you’ll feel better as a result.
Take care of yourself in small ways. Small changes can make a big difference in how you feel. Manage stress during the day by closing your eyes for 15 seconds and taking a few deep breaths. Try to eat more healthfully by adding a vegetable to two of your meals during the day. Turn off the television and your electronic devices an hour before you go to bed to help you get the rest you need.
Preview a skill online before you pay to take a class. In a rapidly changing world, all of us need to keep updating our skills to meet new work and other realities. But going back to school can be expensive and time consuming. Before you invest a substantial amount of money in a class, try to preview a skill online. Watch or listen to any of the hundreds of thousands of videos or podcasts on an infinite number of topics that you can preview by downloading or streaming them. Watch them while you’re commuting, or listen to them while you walk. If you want or need more help than the video or podcast provides, invest in a class
Collect ideas for vacations — then take one. Taking a break to reenergize is more important than ever in our on-the-go world. And many people don’t take vacations just because they don’t know where to go. It takes some research to find a destination that you can afford, and some of us don’t do this until it’s too late. To get inspired, keep a jar or small box where you can store vacation ideas. Every time you hear a friend or relative talk about a wonderful vacation, write down what appeals to you about it and put it there. When you read an article about a place that sounds interesting, put that in the box or jar, too. Once a year, pick a destination from all of the vacation ideas you’ve accumulated.
Get things done while you’re enjoying family and friends. Cook dinner with your kids. When you prepare a meal together, you’re also spending time together. Take a walk with your close friend before work or a tae kwon do class with your partner on the weekend. You’ll be exercising while spending quality time together. At holiday times, plan a cookie exchange and donate some of the cookies to a women’s shelter.
Have 10 technology-free minutes each day with your children. Give the kids time when you aren’t distracted by electronic gadgets. Sit on the floor and do a puzzle. Ask teenagers how their day went, and just listen. Check your email only at certain times of the day, so you aren’t always on it when children need you. When you’re on the phone, turn around and face away from your computer so you aren’t distracted by email. Looking away from the screen will force you to pay attention to the person you’re talking with.
Plan for future caregiving responsibilities. Get a head start if you’re taking care of a grandparent or may be caring for a parent or other relative in the future. Sit down with the adults in your life who may require care. Try to clarify what they want, understand their financial resources, and come up with a plan for meeting their needs and wishes. Try to include in the meeting any family and friends who form a broader network of care, so you don’t have to do it all on your own. Don’t wait for a crisis.
Keep on top of everyday maintenance. Clean as you go, so the work doesn’t pile up. Put a load of laundry in the washing machine in the morning before you leave for work, and put it in the dryer when you get home. Keep a small bucket of cleaning supplies in the bathroom, and wipe down the shower, mirror, and toilet every morning. Set a timer for 10 minutes each weekend and assign each member of your family a task — vacuuming, dusting, straightening up. Check the owner’s manual of your car for the recommended maintenance schedule and write it on your calendar.
Free, confidential counseling for employees of AAA member organizations.
LifeWorks is your employee assistance program (EAP) and well-being resource. We’re here for you any time, 24/7, 365 days a year, with expert advice, resources, referrals to counseling, and connections to specialists including substance abuse and critical incident stress management professionals. If you could benefit from professional help to proactively address a personal or work-related concern, you can turn to LifeWorks.
Counseling is available at no cost to you. (Up to three sessions per issue.)
To meet individual needs and preferences, counseling is available face-to-face AND live by video.
All our counselors are experienced therapists with a minimum Master’s degree in psychology, social work, educational counseling, or other social services field.
Call LifeWorks, toll-free, 24/7, at 800-929-0068. Visit us online at login.lifeworks.com or by
mobile app (username: theaaa; password: lifeworks)
CMS Announces Revisions to Provider Enrollment Moratoria Access Waiver Demonstration (PEWD) Program
On August 20, 2018, the Centers for Medicare & Medicaid Services (CMS) published a notice in the Federal Register that it would be revising the terms of its Provider Enrollment Moratoria Access Waiver Demonstration (PEWD) Program. These revisions became effective on August 20, 2018.
Section 6401(a) of the Affordable Care Act granted CMS the authority to impose temporary moratoria on the enrollment of new Medicare providers and suppliers to the extent doing so was necessary to combat fraud or abuse. Based on this authority, CMS has implemented temporary moratoria on the enrollment of new non-emergency ambulance providers in the states of New Jersey and Pennsylvania.
Under the Provider Enrollment Moratoria Access Waiver Demonstration (PEWD) Program, CMS has the authority to grant waivers to statewide enrollment moratorium on a case-by-case basis in response to access to care issues. However, since the implementation of the PEWD Program in 2016, CMS has identified a handful of technical issues that have complicated the implementation of the PEWD Program. The revisions in this notice are intended to resolve these technical issues.
The specific revisions CMS is making include:
In December 2016, Congress enacted the 21st Century Cures Act. Section 17004 of that law prohibits payment for items or services furnished within moratoria areas by any newly enrolled provider or supplier that falls within a category of health care provider that is subject to the enrollment moratoria. This provision became effective on October 1, 2017. CMS is revising the PEWD Program to waive the requirements of Section 17004 of the Cures Act with respect to providers and suppliers who were granted waivers under the PEWD.
CMS is further revising the PEWD to create a second category of waivers for those providers or suppliers that had submitted an enrollment application prior to the implementation of the moratoria, but who were denied as a result of the implementation of the moratoria. CMS indicated that this new waiver authority was necessary to protect providers and suppliers that spent substantial amounts of time and money preparing for enrollment at the time the enrollment moratoria were county-based, only to be denied once the moratoria were expanded to the entire state.
CMS is revising the PEWD to provide additional discretion regarding the effective date of billing privileges for providers and suppliers granted waivers under the PEWD.
The AAA continues to press policy initiatives with Congress and the Administration that are important to our members. While not as high-profile as our successful efforts earlier this year on the five-year extension of the Medicare ambulance add-ons, the AAA is working hard on ambulance legislation and regulations that impact the EMS industry and ambulance services across the country. Here is a snapshot of those current efforts. Over the next month, we will be providing weekly in-depth updates highlighting these issues.
Ambulance Cost Data Collection System
The AAA was successful in getting our preferred language of an ambulance cost data collection system using a survey and random sample methodology included with the extension of the add-ons in the Bipartisan Budget Act of 2018. However, that was just the first key step in the process. We now need to ensure that CMS gets the details right as the agency develops the structural specifics and data elements for the system. It is critical that the system is designed in a way that ambulance service suppliers and providers will submit the most accurate data possible.
The data will ultimately provide the information necessary for Congress, the Centers for Medicare and Medicaid Services (CMS) as well as the AAA and other stakeholders to reform the Medicare ambulance fee schedule. Reform will include potential reimbursement for services such as community paramedicine, treat and refer, and other items that don’t involve transporting the patient. However, in order to determine the reimbursement levels, we first need the data on what it could cost for these additional services. The AAA therefore has been working closely with officials at CMS on the development of the data collection system.
Medicare Community Bill
The five-year extension of the add-ons and authorization of data cost collection system were the first steps needed in the long-term goal of reforming the Medicare ambulance fee schedule. The AAA is now developing the next piece of legislation as step two of the process. The “Community Bill” would make the Medicare ambulance add-ons permanent, treat ambulance service suppliers like providers in three specific instances, direct the Centers for Medicare and Medicaid Services (CMMI) to do additional pilot programs on innovative services being done by ambulance agencies, reduce regulatory burdens, and implement a more accurate definition of what Goldsmith Modification zip codes should remain as rural. The AAA is currently developing the draft bill and reaching out to congressional offices regarding the introduction of the bill which will likely occur early next Congress.
Restructuring of Dialysis Offset
The AAA is supporting the efforts of our members who would be significantly adversely affected by the upcoming reduction in dialysis transport reimbursement to restructure the cut. Congress included in the Bipartisan Budget Act of 2018 an offset to go along with the extension of the add-ons that will cut reimbursement for BLS nonemergency transports to and from dialysis centers by an additional 13%. This will be on top of the existing 10% reduction. The NEATSA Act (H.R.6269) by Congressman LaHood (R-IL) and Congresswoman Sewell (D-AL) would restructure the offset so that a majority of the additional reduction would be focused on those ambulance service agencies in which 50% or more of their volume are repetitive BLS nonemergency transports. The cut is currently scheduled to be implemented on October 1 and impacted AAA members and the AAA are working to get a Senate companion bill introduced shortly.
Rural EMS Grant Program
As an amendment to the Farm Bill (S. 3042) that passed the Senate, Senator Dick Durbin (D-IL) included language similar to the SIREN Act (S. 2830, H.R. 5429) to reauthorize the Rural EMS Grant program. However, in an effort to ensure the funding would go to the most needy, small, and rural EMS providers, the language of the amendment and SIREN Act would change the eligibility to just governmental and non-profit EMS agencies. Therefore, small rural for-profit ambulance service providers would no longer be eligible to apply for grants.
The AAA is pressing Senator Durbin as well as other members supportive of the reauthorization to revise the language to ensure small rural for-profit providers would still be able to apply for grants. In the next few weeks, the AAA will be asking AAA members to reach out to their members of Congress in support of the final Farm Bill including the reauthorization language and that it continues to also apply to for-profit providers as well.
Easing Regulatory Burdens
Over the last year, the AAA has responded to several requests for information from CMS as well as Congress on how to ease regulatory burdens for Medicare providers and suppliers. In addition to these broader opportunities, representatives of the AAA and our members have been meeting with CMS officials to reduce burdens for our industry. As a specific example, we are pushing for the elimination of the PCS for interfacility transports and to expand the categories of facility personnel eligible to sign the form.
Protecting Non-Emergency Ambulance Services
The AAA continues to educate members of Congress and congressional staff about the importance of non-emergency ambulance services. We are providing congressional offices with a clearer picture as to the vital role of these transports as part of the overall health care system. We are also looking to ensure that changes in federal payor policies strengthen the role and distinction of non-emergency ambulance transports from non-medical transportation services to health care facilities.
Zip Code Changes
The current use of Rural-Urban Commuting Areas (RUCA) as the basis of the Goldsmith Modification for determining rural areas in larger urban counties needs to be reformed. There are numerous examples of zip codes that are designated as urban under the Medicare ambulance fee schedule that are clearly rural. The AAA Rural Task Force is leading the way on both short-term and long-term efforts to more accurately capture rural zip codes in large urban counties. The AAA will include the ultimate reform provision crafted by the Task Force within the Community Bill as well as look at other legislative opportunities to make the changes.
Questions?: Contact Us
If you have questions about the legislation or regulatory initiatives being undertaken by the AAA, please do not hesitate to contact a member of the AAA Government Affairs Team.
Tristan North – Senior Vice President of Government Affairs tnorth@ambulance.org | (703) 610-0216
Ruth Hazdovac – AAA Senior Manager of Federal Government Affairs rhazdovac@ambulance.org | (703) 610-5821
Aidan Camas – Manager of State & Federal Government Affairs acamas@ambulance.org | (703) 610-9039
Thank you for your continued membership and support.
Talking Medicare: Recent DOJ Settlement Highlights Importance of Exclusion Testing
On July 17, 2018, the U.S. Attorney for the District of Maine issued a press release on a settlement that had been reached with an ambulance service in Maine. As a result of this settlement, the ambulance service agreed to pay $16,776.74 to resolve allegations that it had submitted false claims to the Medicare and Maine Medicare Programs.
While the Department of Justice’s press release referred to the matter as a civil health care fraud, that headline is somewhat misleading. The ambulance service was not alleged to “up-coded” its claims or to have billed for patients that did not require ambulance transportation. Rather, the ambulance service was accused of using monies paid to it by these federal health care programs to pay the salary and benefits of a woman hired to assist the company’s billing manager. The woman, who was not identified in news reports, had previously been excluded from participation in federal health care programs after surrendering her license as a pharmacy technician after being found to have inappropriately diverted certain controlled substances. The ambulance service apparently failed to conduct an exclusion test on this individual prior to placing her on its payroll. The ambulance service’s side of the story is discussed in greater detail in this article from the local newspaper.
This settlement provides a reminder of the potential liabilities associated with the employment excluded individuals. As the HHS Office of the Inspector General (OIG) noted in its May 2013 Special Advisory Bulletin, the effect of exclusion goes beyond direct patient care. The OIG noted that excluded individuals are prohibited from providing transportation services paid by a federal health care program, using the example of ambulance drivers and ambulance dispatchers. The OIG further indicated that excluded individuals cannot provide administrative and/or management services that are payable by federal health care programs, even if these administrative or management services are not separately billable. In the above-referenced case, the prohibition was applied to the wages and benefits payable to the excluded employee.
Do we need to conduct exclusion testing, and, if so, how frequently?
The OIG recommends that all health care providers conduct exclusion testing prior to an individual’s employment, and then periodically thereafter. However, the OIG takes no formal position on how frequently these periodic exclusion checks should be conducted. The OIG does note, however, that it updates its List of Excluded Individuals and Entities (LEIE) on a monthly basis.
Given the potential risks involved, I think monthly testing of all employees should definitely be considered a best practice. The hope is that this case serves as a cautionary tale for other ambulance providers.
Have an issue you would like to see discussed in a future Talking Medicare blog? Please write to me at bwerfel@aol.com.
CMS Extends Temporary Moratorium on Non-Emergency Ground Ambulance Services in New Jersey and Pennsylvania
The Centers for Medicare & Medicaid Services (CMS) has announced that it intends to extend the temporary moratoria on the enrollment of new Medicare Part B non-emergency ground ambulance providers and suppliers in the states of New Jersey and Pennsylvania. The extended moratoria will run through January 29, 2019. Notice of the extension of the temporary moratorium will appear in the Federal Register on August 2, 2018.
Section 6401(a) of the Affordable Care Act granted CMS the authority to impose temporary moratoria on the enrollment of new Medicare providers and suppliers to the extent doing so was necessary to combat fraud or abuse. On July 31, 2013, CMS used this new authority to impose a moratorium on the enrollment of new ambulance providers in Houston, Texas and the surrounding counties. On February 4, 2014, CMS imposed a second moratorium on newly enrolling ambulance providers in the Philadelphia metropolitan areas. These moratoriums were subsequently extended on August 1, 2014, February 2, 2015, July 28, 2015, and February 2, 2016.
On August 3, 2016, CMS announced changes to the moratoria on the enrollment of new ground ambulance suppliers. Specifically, CMS announced that: (1) the enrollment moratoria would be lifted for the enrollment of new emergency ambulance providers and supplier and (2) the enrollment moratoria on non-emergency ambulance services would be expanded to cover the entire states of New Jersey, Pennsylvania, and Texas. At the same time, CMS announced the creation of a new “waiver” program that would permit the enrollment of new non-emergency ambulance providers in these states under certain circumstances. The revised moratorium on newly enrolling non-emergency ground ambulance providers was subsequently extended on January 9, 2017 and July 28, 2017.
On September 1, 2017, CMS issued a notice on its website indicating that it had elected to lift the moratorium on the enrollment of new Part B non-emergency ambulance suppliers in Texas, effective September 1, 2017. CMS indicated that this decision was made to assist in the disaster response to Hurricane Harvey. CMS published formal notice of the lifting of this moratorium on November 3, 2017.
On January 30, 2018, CMS announced an extension of the moratorium on the enrollment of new Part B non-emergency ambulance suppliers in New Jersey and Pennsylvania.
CMS will need to make a determination on whether to extend or lift the enrollment moratorium on or before January 29, 2019.
CMS Issues Data Elements and Templates for Non-Emergency Ambulance Transports (NEAT): Open Door Forum for
Thursday, July 26, 2018 Just Announced
As part of its Patients Over Paperwork Project, the Centers for Medicare & Medicaid Services (CMS) Provider Compliance Group (PCG) has been hosting quarterly listening sessions and reviewing the Request for Information submissions. The American Ambulance Association has been actively engaged in these efforts, highlighting the recommendations we submitted to CMS and the House Ways & Means Committee last year. These recommendations included suggestions as to how CMS could streamline regulatory requirements to eliminate duplicative requirements and reduce regulatory burdens. In addition to these efforts, CMS has been working to standardize documentation data elements and establish templates that providers and suppliers can use to help make the current documentation processes less burdensome as well.
On July 24, CMS released draft documentation-related clinical data elements and clinical templates that could be used for the Physician Certification Statement, Progress Notes, and Prior Authorization requests. View the Documents. These documents are not intended to change current law.
CMS also announced yesterday that it will discuss the templates on a Special Open Door Forum which is scheduled for July 26 at 2-3 pm ET. The call-in information is:
Participant Dial-In Number: 1-(888)-989-4575
Conference ID: 3068545
We have shared our concern about the short notice about the call and CMS has indicated it will continue to take comments on the documents after the call as well. The AAA is in the process of reviewing these documents closely and will develop a written comment letter to provide to CMS after the call on Thursday. We welcome input from all our members as part of this process.
While these new documents may be helpful for many services, the AAA also remains committed to move its recommendations which would result in some changes in the PCS and other ambulance provider and supplier requirements.
In sum, the OIG reviewed claims that Medicare paid for 2014 – 2016 non-emergency ambulance transports. The review focused on transports to non-covered destinations. OIG found that $8,633,940 was paid by Medicare for non-emergency ambulance transports under codes A0425 (ground mileage), A0426 (ALS non-emergency) and A0428 (BLS non-emergency) during this period of time.
The review was based solely on the claims and not based on a medical review or interviews of providers.
The claims that should not have been paid were to the following destinations:
59% – to diagnostic or therapeutic sites other than a hospital or physician’s office, that did not originate at a SNF.
31% – to a residence or assisted living facility (and not meeting the origin/destination requirement).
6% – to the scene of an acute event.
4% – to a destination code not used for ambulance claims or where no destination modifier was used.
<1% – to a physician’s office.
OIG recommended (and CMS agreed) that CMS:
Notify the Medicare Administrative Contractors to recover that portion of the overpayment that is within the 4-year period in which claims can be re-opened.
For the balance of the overpayment that is outside the 4-year period, CMS should provide the information needed for the MACs to notify the providers of the overpayments and have the providers exercise reasonable diligence to investigate and refund improper payments.
Direct the MACs to review the origin/destination requirements for any overpayments following the audit period.
Require the MACs implement edits to ensure they only pay for non-emergency transports that meet the Medicare requirements.
There is a chart in the report that indicates the improper payments for each jurisdiction. It is interesting to note that the overpayments range from a low of $515 (First Coast) to a high of $5,006,696 (Cahaba).
On Thursday, July 12, the Centers for Medicare & Medicaid Services (CMS) released the “Revisions to Payment Policies under the Physician Fee Schedule and Other Revisions to Part B for CY 2019; Medicare Shared Savings Program Requirements; Quality Payment Program; and Medicaid Promoting Interoperability Program” Proposed Rule (Proposed Rule).
As you know, the American Ambulance Association worked closely with the Congress to ensure passage of the Bipartisan Budget Act of 2018 (BBA) (Pub. L. 115-123, enacted on February 9, 2018). The BBA not only extended the ambulance add-ons for 5 years, but also authorized a cost collection system that would not be overly burdensome on ambulance providers and suppliers, but would provide sufficient information ideally to support the permanent extension of the add-ons and set the basis for new payment models, including alternative destinations, treatment/assessment without transport, and community paramedicine.
After passage of the BBA, the AAA engaged immediate with CMS to ensure the smooth implementation of these provisions. Those contacts resulted in guidance earlier this year implementing the add-ons retroactively to January 1, 2019.
Consistent with the statute and already-released guidance, the Proposed Rule extends the three add-ons: the 2 percent urban, 3 percent rural, and 22.6 percent super-rural add-ons. The Proposed Rule would codify the extension of the add-ons through December 31, 2022.
The Proposed Rule would implement the increase in the reduction in rates for non-emergency ambulance transports to/from dialysis facilities for services furnished on or after October 1, 2018. The 10 percent reduction applies for these transports furnished during the period beginning on October 1, 2013 and ending on September 30, 2018. The reduction will increase to 23 percent to conform the regulations to the statutory requirement for services furnished on or after October 1, 2018.
CMS does not request any information about the cost collection system in the Proposed Rule, but has been soliciting comments and recommendations through informal provider/supplier calls. Additionally, the AAA has been in regular contact with CMS on the structure, design, and data elements to ensure the successful implementation of this critically important system as well.
Talking Medicare: GAO urges CMS to continue prior authorization efforts
On May 21, 2018, the Government Accountability Office (GAO) issued a report to the U.S. Senate Finance Committee on the use of prior authorization models by the Centers for Medicare and Medicaid Services (CMS). The GAO was asked to examine: (1) the impact of prior authorization on total expenditures, and the potential savings for items or service subject to prior authorization, (2) the reported benefits and challenges of prior authorization, and (3) CMS’ monitoring of these programs, and its plans for future prior authorization. To conduct its study, the GAO looked at payment data and other information provided by CMS. The GAO also interviewed CMS, the Medicare Administrative Contractors (MACs), and selected provider, supplier, and beneficiary groups.
Prior authorization was first implemented by CMS in 2012 for certain power mobility devices (e.g., power wheelchairs) in seven states. Subsequent prior authorization models were implemented for non-emergency hyperbaric oxygen and home health services. Most relevant to our industry, CMS implemented a prior authorization model for repetitive, scheduled, non-emergency ambulance transportation in December of 2014. Originally, this model was implemented in only three states: New Jersey, Pennsylvania, and South Carolina. In January of 2016, the prior authorization model was expanded to include the states of Delaware, Maryland, North Carolina, Virginia, and West Virginia, as well as the District of Columbia.
The GAO’s key finding is that these prior authorization models have been effective in reducing Medicare’s expenditures for various items. The GAO’s analysis of actual expenditures found that the estimated savings from all demonstrations through March of 2017 could be as high as $1.1 to $1.9 billion. Given this fact, it should not be surprising that the GAO is calling on CMS to continue the use of prior authorization.
The majority of the data included in this report relates to non-ambulance services. However, I do want to highlight a few data points noted by the GAO.
From the model’s implementation in December 2014 through March 2017, MACs collectively handled more than 337,000 prior authorization requests, including a total of 3,231 requests for authorization of a repetitive, non-emergency, ambulance patient. This includes 2,620 initial requests, and 611 resubmissions (i.e., subsequent requests for prior authorization following the rejection of the initial request).
The GAO provisional affirmation rate for both initial and resubmitted authorization requests rose in each demonstration between the initial implementation date and March 2017. For example, the GAO noted that the affirmation rate (i.e., the rate at which patients are approved for repetitive ambulance transportation) during the first six months of the non-emergency ambulance model was 28 percent. This rose to 66 percent during the most recent six-month period (October 2016 through March 2017). The GAO noted that MAC officials attributed this increase, in part, to provider and supplier education, which they felt improved the documentation being submitted by providers and suppliers. While this is undoubtedly true, it is also likely the case that the MACs refined their approval process over time.
The GAO estimated the total potential savings from the prior authorization model for ambulance to be nearly $387.5 million from December 2014 through March 2017. Importantly, 90 percent of that savings was attributable to reductions in utilization in the original three states. Moreover, more than half the reduced expenditures took place within the first six months of the demonstration project.
In terms of fitting this report into the larger picture, I think it is best viewed as further confirmation of what we already suspected: namely, that the federal government perceives prior authorization to be an effective tool for combating the perceived overutilization of ambulance to transport patients to and from dialysis. CMS indicated as much when it adopted the program in 2014. Medicare payment data has borne out those expectations. Recently, CMS issued its first interim report on prior authorization’s effectiveness. The GAO’s report adds an independent imprimatur to that belief.
Big picture, all of the stars appear to be lining up for an expansion of prior authorization next year. Stay tuned!!
Have an issue you would like to see discussed in a future Talking Medicare blog? Please write to me at bwerfel@aol.com.
The AAA would like to take this opportunity to update members on a number of issues related to Medicare reimbursement:
CMS and its contractors have begun adjusting claims for ground ambulance services to reflect the restoration of the temporary add-ons. Section 50203(a) of the Bipartisan Budget Act of 2018 retroactively reinstated the temporary add-ons for ground ambulance services. These add-ons increase the applicable Medicare allowables by 2% in urban areas, 3% in rural areas, and 22.6% in “super rural” areas (over and above the corresponding rural rate), retroactive to January 1, 2018. On a March 7, 2018 Open Door Forum, CMS indicated that it had updated the Medicare Ambulance fee schedule to reflect these higher rates, and that it has provided a Change Request to each of its Medicare Administrative Contractors (MACs). The AAA has confirmed that all MACs have successfully implemented the new rates, and that all are paying current claims at the correct rate. The AAA has further confirmed that MACs have started to adjust 2018 claims paid at the original (lower) rates. Unfortunately, neither CMS nor its MACs have committed to a firm timetable for the completion of all required adjustments; however, a number of MACs have indicated that they anticipate completing all required adjustments by the end of the second quarter of 2018.
Further reduction in Medicare’s payment for non-emergency BLS transports to and from dialysis. The Bipartisan Budget Act of 2018 further required CMS to implement an additional 13% reduction in Medicare’s payment for scheduled, non-emergency BLS transports to and from dialysis. This reduction is on top of the existing 10% payment reduction. Collectively, this means that dialysis transports will be reimbursed at a rate that is 23% less than the rate that would otherwise be applicable to BLS non-emergency transports in your area. The AAA. is reminding members that this additional reduction in payments will go into effect for transports on or after October 1, 2018.
CMS has updated its SNF Consolidated Billing file to resolve the error that resulted in certain ambulance claims being incorrectly denied as being the responsibility of the SNF. Each year, CMS updates the SNF Consolidated Billing file provided to MACs. This file contains several lists of Healthcare Common Procedure Coding System (HCPCS) codes, and provides instructions to the MACs on whether these codes: (i) should be accepted for separate payment under Medicare Part B or (ii) should always be denied for inclusion in the SNF Consolidated Billing system. Ambulance HCPCS codes (A0425, A0426, A0427, etc.) have always been included in the first list, as the issue of whether an ambulance transportation is bundled to the SNF is conditioned on the nature of the services that the patient will receive at the destination. To the extent the service the patient will receive at the destination is bundled, the ambulance services to and from that service will also be bundled, and vice versa. Note: there are two exceptions to this general rule. The first is that ambulance transportation to and from dialysis is specifically exempted from the SNF Consolidated Billing regime, and therefore will always be separately billable to Medicare Part B. The second exception relates to the provision of chemotherapy services furnished on an outpatient basis in a hospital. Chemotherapy services are generally bundled to the SNF; however, several years ago, Congress elected to exempt a number of particularly expensive forms of chemotherapy from the SNF bundle. In these instances, while the SNF is not responsible for the payment of the expensive chemotherapy, the SNF remains responsible for payment of the ambulance transportation to and from the hospital. Because ambulance codes may or may not be bundled to the SNF based on the nature of the transport, they are not automatically denied. Instead, the MACs are supposed to use further edits to identify those situations in which the ambulance transport would be bundled vs. separately payable. Unfortunately, in its 2018 update, CMS inadvertently left the ambulance HCPCS codes off the list of codes that are not automatically denied as being bundled to the SNF. As a result, ambulance providers have indicated that claims were being denied using remark code “OA109.” In some cases, claims for dates of service in 2016 or 2017 that were previously paid were being recouped. CMS recognized its error fairly quickly, and updated the SNF Consolidated Billing file in mid-February. All MACs were provided with updated instructions by February 27, 2018. Therefore, the issue has been resolved for current claims. What remains to be resolved is how CMS and its MACs will adjust or reprocess claims that were incorrectly denied. Several MACs have notified providers of the issue, and asked that they refrain from appealing the claims. These MACs are indicating that they will automatically adjust/reprocess affected claims. In other instances, the MACs have asked the providers to make a refund of affected claims that were previously paid, promising to then reprocess the entire claim. The AAA is advising members to carefully track the claims that were affected by this mistake, and to follow the instructions issued by their MAC for ensuring their reprocessing.
CMS has delayed the mailing new ID cards to all Medicare beneficiaries. As part of the Medicare Access and CHIP Reauthorization Act of 2015, Congress mandated that CMS remove a beneficiary’s social security number (SSN) from their Medicare ID card by April 2019. As part of this initiative, CMS will be replacing the SSN-based Health Insurance Claim Number (HICN) with the new Medicare Beneficiary Identifier (MBI). CMS has already started mailing cards with the MBI to newly enrolling Medicare beneficiaries. CMS originally announced that it would be mailing new cards to existing Medicare beneficiaries starting in April 2018, but recently indicated that it would delay the mailing of new cards to existing Medicare beneficiaries until May 2018. From May to June, CMS will mail new cards to existing Medicare beneficiaries residing in Alaska, California, Delaware, Hawaii, Maryland, Oregon, Pennsylvania, Virginia, West Virginia, the District of Columbia, and the U.S. territories of American Samoa, Guam, and the Northern Mariana Islands. The mailing program will then be extended to additional states in 5 “waves” over the coming year. To the extent you provide services in the above-mentioned states, you may want to educate crewmembers and other employees on the differences between the HICN and the MBI. You may want to also consider updating your existing patient databases to include the new identifier. As a reminder, CMS will permit claims to be submitted with either the HICN or the MBI during a transition period running through December 31, 2019. Effective January 1, 2020, claims must be submitted with a patient’s MBI. This requirement applies regardless of whether the date of service occurred prior to the expiration of the transition period.
Extension of prior authorization project for scheduled, repetitive transports. In December 2017, CMS indicated that it would be extending the prior authorization program for an additional year. This program is currently in place for the states of Delaware, Maryland, New Jersey, North Carolina, Pennsylvania, South Carolina, Virginia, West Virginia, and the District of Columbia. The extension of the program is limited to those states. CMS has further indicated that it will be making a determination on possible national expansion at some point in the near future. CMS recently released its first interim report on the prior authorization program. As expected, that report indicated that prior authorization has been successful in reducing Medicare expenditures on scheduled, repetitive transports, without any material impact on beneficiary access to and quality of care.
Have any questions about these updates? Contact Brian Werfel at bwerfel@aol.com
CMS held its latest Open Door Forum on Wednesday, March 7, 2018. As with past Open Door Forums, CMS started the call with the following series of announcements:
Medicare Fee Schedule – CMS indicated that the Bipartisan Budget Act of 2018, enacted on February 9, 2018, contained several provisions that impacted the payment of ambulance claims under the Medicare Ambulance Fee Schedule:
Temporary Add-Ons for Ground Ambulance – CMS indicated that Section 50203(a) of the bill extended the temporary add-ons for ground ambulance services for an additional five years, retroactive back to January 1, 2018. As extended, these add-ons will expire on December 31, 2022. These add-ons increase Medicare’s allowable for ground ambulance base rates and mileage by 2% in urban areas, 3% in rural areas, and by 22.6% (over the applicable rural rate) for services provided in so-called “super rural” areas.
Cost Reporting – CMS indicated that Section 50203(b) of the bill would require ground ambulance providers and suppliers to submit cost data to CMS. CMS noted that the new law requires CMS to develop, no later than December 31, 2019, a data collection system to collect cost, revenue, utilization, and certain other information related to ground ambulance services. The law provides that cost data will be collected using a survey methodology, with a representative sample of ambulance providers and suppliers being asked to submit cost data in any given year. Finally, CMS noted that, starting on January 1, 2022, providers or suppliers that fail to submit the requested cost data would be subject to a 10% reduction in their Medicare payments, unless otherwise exempted on the basis of significant hardship.
Additional Reduction in Medicare Payment for Dialysis Transports – Section 53108 of the bill provides that the Medicare allowable for non-emergency, basic life support transports to and from dialysis will be subject to a further 13% reduction. This reduction would go into effect for dialysis transports with dates of service on or after October 1, 2018. This would be on top of the existing 10% reduction in Medicare’s payment for dialysis transports, for a total reduction of 23%.
Temporary Enrollment Moratorium – CMS indicated that the temporary moratorium on the enrollment of new ground non-emergency ambulance providers in Texas was lifted on September 1, 2017. CMS further indicated that the enrollment moratorium was extended for the states of New Jersey and Pennsylvania for an additional six months on January 29, 2018. CMS will need to make a determination on or before July 29, 2018 on whether to lift the moratorium or extent it for an additional six months in that state.
Following the announcements, CMS moved into a brief Question & Answer period. Most of the questions were not answered on the call; instead, CMS took the contact information of the person asking the question, and indicated that they would respond directly to them at a later date. However, the following questions were answered:
CMS indicated that a Change Request had been sent to all Medicare Administrative Contractors (MACs) informing them of the new, adjusted fee schedule amounts. CMS further indicated that this Change Request, which it indicated was confidential, provided further instructions to the MACs on when and how to adjust claims initially paid at the original 2018 rates.
CMS confirmed that the adjusted rates are retroactive to January 1, 2018. Accordingly, CMS indicated that claims paid at the original 2018 rates will be adjusted by the MACs at some future date.
CMS indicated that it recently released its First Interim Evaluation Report on the Medicare Prior Authorization Model for repetitive, non-emergency ground ambulance transports. CMS further indicated that it was still reviewing this report, and that no decision has yet been made on the extension of this model within the existing 9 states and the District of Columbia and/or the expansion of the model to additional states.
Have questions? Please write to the Werfels at bwerfel@aol.com.
CMS Posts Updated 2018 Public Use File; OIG Guidance on Waiver of Small Cost-Sharing Balances Updated AAA 2018 Medicare Rate Calculator Now Available!
The Centers for Medicare and Medicaid Services (CMS) has posted an updated version of the 2018 Medicare Ambulance Fee Schedule Public Use Files (PUF). These files contain the Medicare allowed base rate reimbursement amounts for the various levels of ambulance service and mileage rates. These files reflect the restoration, retroactive to January 1, 2018, of the temporary add-ons for ground ambulance services (2% for urban transports, 3% for rural transports, and the “super-rural” bonus) pursuant to the Bipartisan Budget Act of 2018, which was enacted on February 9, 2018.
The American Ambulance Association has reviewed the rates in this file and confirmed that the rates are accurate. The AAA has also revised its Medicare Ambulance Rate Calculator to reflect the five-year extension of the ambulance add-ons as well as other policy changes including the two-year extension (2026 and 2027) of the 2% Medicare provider cut under sequestration and the additional 13% (23% total) cut to BLS nonemergency transports to and from dialysis centers. The additional dialysis transport cut takes effect on October 1, and as a modifier, is not included in the Public Use File.
Unfortunately, CMS has elected in recent years to release its Public Use Files without state and payment locality headings. As a result, in order to look up the rates in your service area, you would need to know the CMS contract number assigned to your state. This is not something ambulance services would necessarily know off-hand. For this reason, the AAA has created a reformatted version of the CMS Medicare Ambulance Fee Schedule, which includes the state and payment locality headings. Members can access this reformatted fee schedule on the AAA website.
CMS has yet to announce a timetable for adjusting claims that were paid at the original fee schedule amounts. It is anticipated that CMS will make an announcement on this timetable in the next few weeks.
Coinsurance
One issue that frequently arises in these situations is how ambulance providers and suppliers should treat the additional coinsurance amounts that are generated when CMS and its contractors adjust claims from the original allowed amounts to the now higher allowed amounts. These additional coinsurance amounts are typically quite small. Ambulance providers and suppliers may determine that the costs associated with trying to collect these small amounts would likely exceed the amounts they could reasonably hope to collect. The question is whether writing off these small balances could be construed as a routine waiver of cost-sharing amounts, a practice prohibited under Medicare’s rules.
In 2010, the HHS Office of the Inspector General (OIG) issued guidance on this issue. Specifically, the OIG indicated that it would not seek to impose administrative sanctions on Medicare providers and suppliers that waive these amounts provided the following conditions are met:
• The waiver is limited to the increased cost-sharing amounts generated upon adjustment of claims previously paid at the lower allowable, i.e., it does not apply to cost-sharing amounts associated with claims paid at the increased allowables;
• The waiver is limited to the small balances created by the adjustment of claims, i.e., it does not apply to the cost-sharing amounts originally imposed on the beneficiary when the claim was paid at the lower amounts;
• The waiver must be offered uniformly to all affected beneficiaries;
• The waiver must not be advertised; and
• The waiver must not be conditioned on the beneficiary’s receipt of any items, suppliers, or services.
Assuming the above-referenced conditions are met, ambulance providers and supplier can safely write-off these small balances. Please note that the OIG is not indicating that ambulance providers and suppliers must write-off these amounts. Rather, the OIG is simply indicating that this is an option available to health care providers and suppliers impacted by retroactive adjustment of claims.