Medicaid Replacement Plans
Medicaid billing in emergency medical services is unavoidable. From trauma trips to non-emergency transports, ambulance providers face a multitude of hurdles when trying to identify, verify and bill the correct payor for Medicaid patients. Guesswork is often used instead of real-time insurance verification.
This can be especially true when commercial payors such as United Healthcare and Blue Cross Blue Shield manage the Medicaid plan, commonly termed Medicaid Replacement Plans. This article provides four valuable tips for successfully processing EMS claims when a Medicaid Replacement Plan is involved.
The Challenge for EMS Billing: Benefits Verification
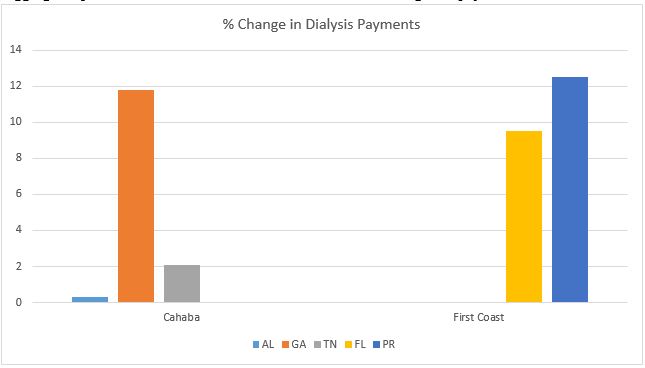
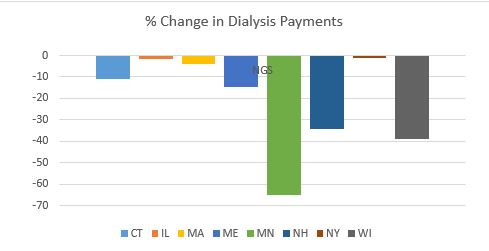
Just as commercial payers see growth opportunities in managing Medicare Advantage (MA) plans, they are also overseeing hundreds of Medicaid programs. According to the annual CMS-64 Medicaid expenditure report, in federal fiscal year (FFY) 2016, Medicaid expenditures across all 50 states and 6 territories exceeded $548 billion, with nearly half of all spending now flowing through Medicaid managed care programs. On average 54.67% of Medicaid dollars are spent on managed care, whether to manage the transition or fund plans. This ranged from 97.9% in Puerto Rico, down to 12.1% in Colorado.
A single trip may have Medicaid benefits, but also managed by United Healthcare or another third-party commercial payer. The result? Blended coverage for Medicaid patients and confusion for providers.
Four Tips to Expedite Medicaid Verification
When checking benefits for Medicaid patients, carefully review the standard eligibility response. Payors usually note benefit management by a commercial payer in the response, but there is no consistency in format or location. The Medicaid Replacement Plan notification may be placed at the top, middle or very bottom of the file. Furthermore, unnecessary additional information may be provided by the payor causing more confusion and time delays for EMS billers. For example, Cigna often includes dental, pharmaceutical and other specialty coverage details even though this information is never required for ambulance trips.
To avoid reimbursement delays with Medicaid Replacement Plans, implement the following four tactics:
Ask the eligibility vendor to place replacement plan information at the top of the file. If notification is placed in the same location and in the same format for every eligibility response, billers save time searching for coverage.
- Request that only pertinent coverage for the claim be included in the eligibility notification. If this is not possible, ask the payer to prioritize eligibility information by placing only the relevant coverage at the top.
- Take time to check and verify eligibility up front. Ensuring a clean and correct claim saves EMS providers back-end expense and expedites reimbursement due to fewer payor rejections and denials.
- Ask your EMS software vendor to integrate eligibility checking directly in your system’s workflow for real-time access during the pre-bill and billing processes. Technology integration saves billing time by eliminating the need to access and enter data into an outside payor portal or insurance discovery application.
Numerous EMS providers struggle with insufficient billing staff to manage claims. Take every step possible to streamline efforts and reduce duplicate work due to denied or rejected claims. When checking eligibility, proper identification and billing of Medicaid Replacement Plans is an essential step.
About the Author:
Stacey Bickford is the Operations and Client Coordinator at Payor Logic. She has been involved with medical billing since a teenager with prior experience in data entry, billing and office management for physicians’ practices, hospitals and especially EMS agencies. Prior to joining Payor Logic in 2016, Stacey started with ZOLL in 2008 as a support technician moving to Product Manager of RescueNet Billing through 2016.
In her free time, Stacey enjoys travelling with her family, Michael and their dogs Benjamin and Poncho. They’ve visited 21 states in the last 15 months! She loves hiking, gardening and being outdoors as much as possible.